Sunday Poster Session
Category: Colon

Mohammed Al-Aquily, MD
Norwalk Hospital/Yale University
Norwalk, CT
Recurrent abdominal pain is a common clinical presentation with a broad differential diagnosis, including anatomical, functional, inflammatory, and infectious causes. One rare etiology is gastrointestinal angioedema, which often presents with colicky, relapsing-remitting abdominal pain. It is a condition characterized by swelling in the submucosal space of the bowel. It is often misdiagnosed and can lead to unnecessary procedures, repeated imaging, and increased healthcare costs due to extensive workup. Intestinal angioedema has multiple causes including food allergies, drug reactions, and hereditary or acquired C1 esterase deficiencies.
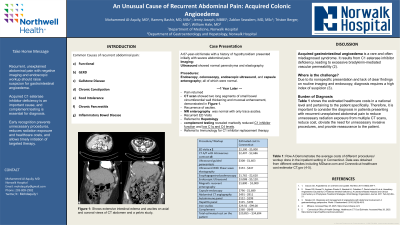
A 67-year-old female with a history of hypothyroidism presented initially with severe abdominal pain. Imaging showed ascites with mildly enlarged liver. Ultrasound showed normal parenchyma and elastography with resolution of ascites. Due to ongoing pain, she had endoscopy, colonoscopy, endoscopic ultrasound, and capsule enterography; all of which were normal. The pain subsided but returned one year later. Repeat CT scan showed two long segments of small bowel circumferential wall thickening and mucosal enhancement, demonstrated in Figure 1. Moderate ascites was again noted. Subsequent MR enterography was normal with only trace ascites. She had multiple other repeated presentations to emergency due to recurrence of the pain, prompting additional CT scans. She was eventually referred to hepatology for evaluation of ascites. Extensive serologic workup was obtained. Ultimately, complement testing revealed markedly reduced C1 inhibitor function and low C1q and C4 levels. She was referred to immunology for initiation of C1 inhibitor replacement therapy.
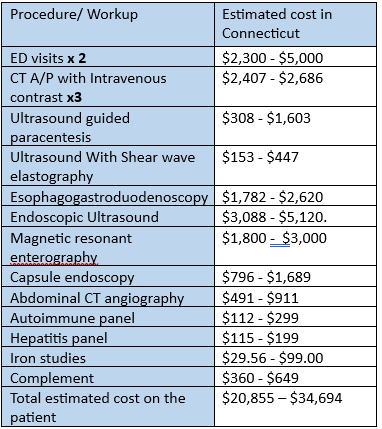
Acquired gastrointestinal angioedema is a rare and often misdiagnosed syndrome. It results from C1 esterase inhibitor deficiency, leading to excessive bradykinin-mediated vascular permeability. Due to its nonspecific presentation and lack of clear findings on routine imaging and endoscopy, diagnosis requires a high index of suspicion. Table 1 shows the estimated healthcare costs in a national level and pertaining to the patient specifically. Therefore, it is important to consider the diagnosis in patients presenting with recurrent unexplained abdominal pain to reduce unnecessary radiation exposure from multiple CT scans, reduce cost, obviate the need for unnecessary invasive procedures, and provide reassurance to the patient.