Sunday Poster Session
Category: Colon
Abdul Wasay, MD
University of Tennessee
Knoxville, TN
A 54-year-old female with a history of esophageal adenocarcinoma, status post-esophagectomy with gastric pull-through and adjuvant chemoradiation (FOLFOX), was started on nivolumab as adjuvant immunotherapy. Four months after initiation, she developed bloody diarrhea with mucus, abdominal pain, urgency, and fatigue, with up to 10–12 bowel movements daily—consistent with grade 3 colitis.
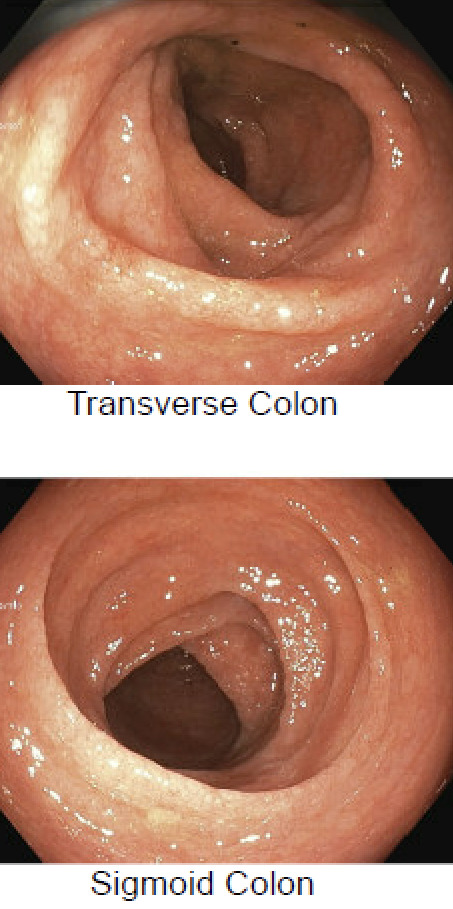
Nivolumab was discontinued, and colonoscopy revealed continuous erythema, friability, and superficial ulceration throughout the colon (Figure 1 and 2). Biopsies demonstrated severe active colitis consistent with ICI-associated colitis, without granulomas, viral inclusions, dysplasia, or malignancy.
She was started on prednisone and infliximab with minimal improvement. Treatment was transitioned to vedolizumab every 8 weeks, which led to partial relief, reducing bowel movements to four per day. A repeat colonoscopy five months later showed diffuse moderate inflammation, and biopsy revealed chronic active colitis. Vedolizumab was increased to every 4 weeks. At two-month follow-up, she reported complete resolution of diarrhea. A follow-up colonoscopy was scheduled six months after dose adjustment to assess response.