
Sunday Poster Session
Category: Colon
Sakshi Bai, MD
Henry Ford Jackson Hospital
Jackson, MI
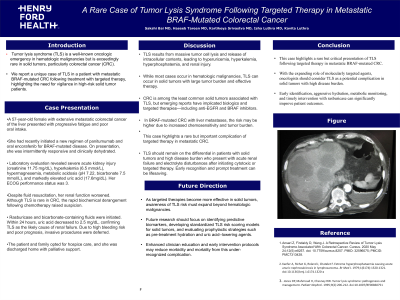
A 57-year-old female with extensive metastatic colorectal cancer to the liver presented with progressive fatigue and poor oral intake. She had recently initiated a new regimen of panitumumab and oral encorafenib for BRAF-mutated disease. On presentation, she was intermittently responsive and clinically dehydrated. Laboratory evaluation revealed severe acute kidney injury (creatinine 11.75 mg/dL), hyperkalemia (6.5 mmol/L), hypermagnesemia, metabolic acidosis (pH 7.22, bicarbonate 7.5 mmol/L), and markedly elevated uric acid (17.6 mg/dL). Her ECOG performance status was 3.
Despite fluid resuscitation, her renal function worsened. Although TLS is rare in CRC, the rapid biochemical derangement following chemotherapy raised suspicion. Rasburicase and bicarbonate-containing fluids were initiated. Within 24 hours, uric acid decreased to 2.5 mg/dL, confirming TLS as the likely cause of renal failure. Her creatinine was consistently around 11mg/dl for several days immediately started to downtrend post initiation of Rasburicase therapy. Due to poor prognosis, invasive procedures were deferred. The patient opted for hospice care, and was discharged home with palliative support.