Sunday Poster Session
Category: Endoscopy Video Forum

Kathryn Thompson, MD
Emory University School of Medicine
Atlanta, GA
Insulinomas are rare neuroendocrine tumors (NET) that cause recurrent fasting hypoglycemia and neuroglycopenic symptoms. Endoscopic ultrasound-guided radiofrequency ablation (EUS-RFA) is a novel, minimally invasive treatment for insulinomas that causes cell death with targeted thermal energy and has been used as an alternative to surgical resection for management of hypoglycemia.
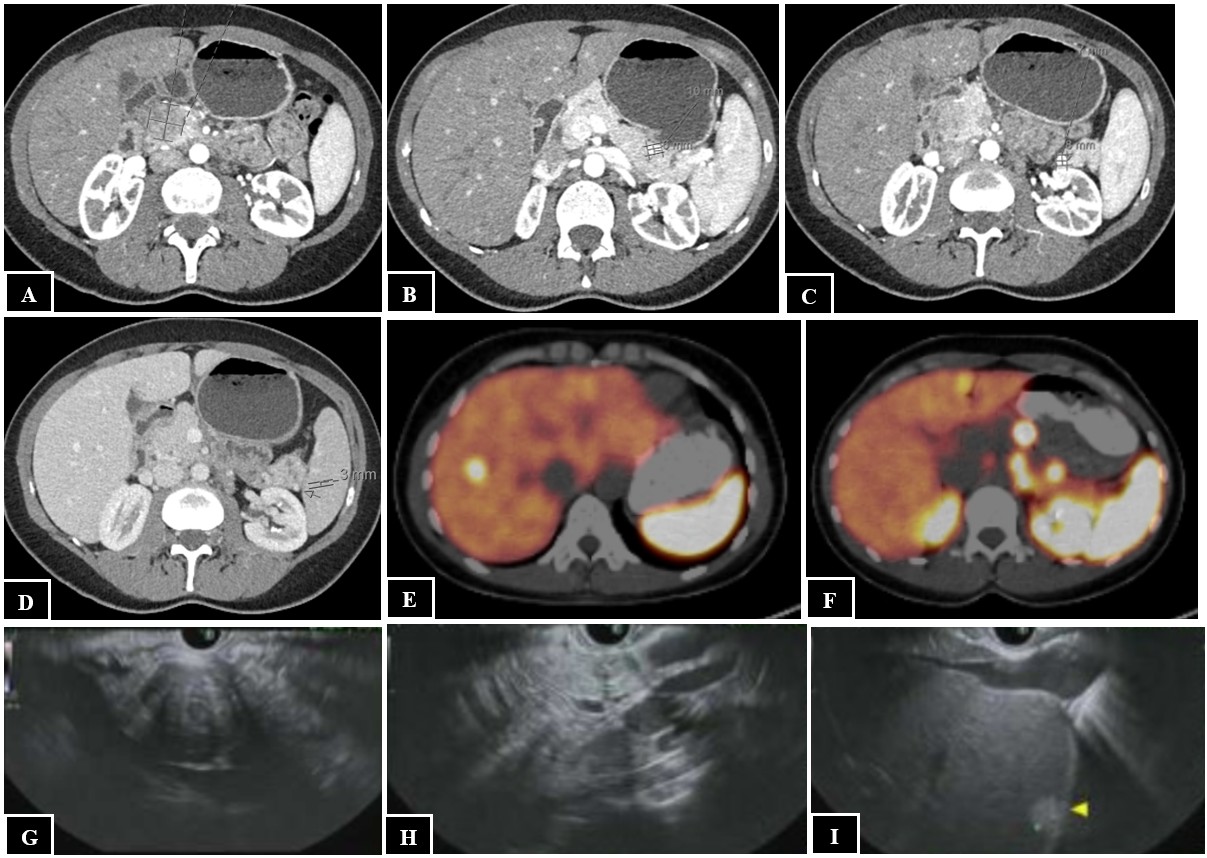
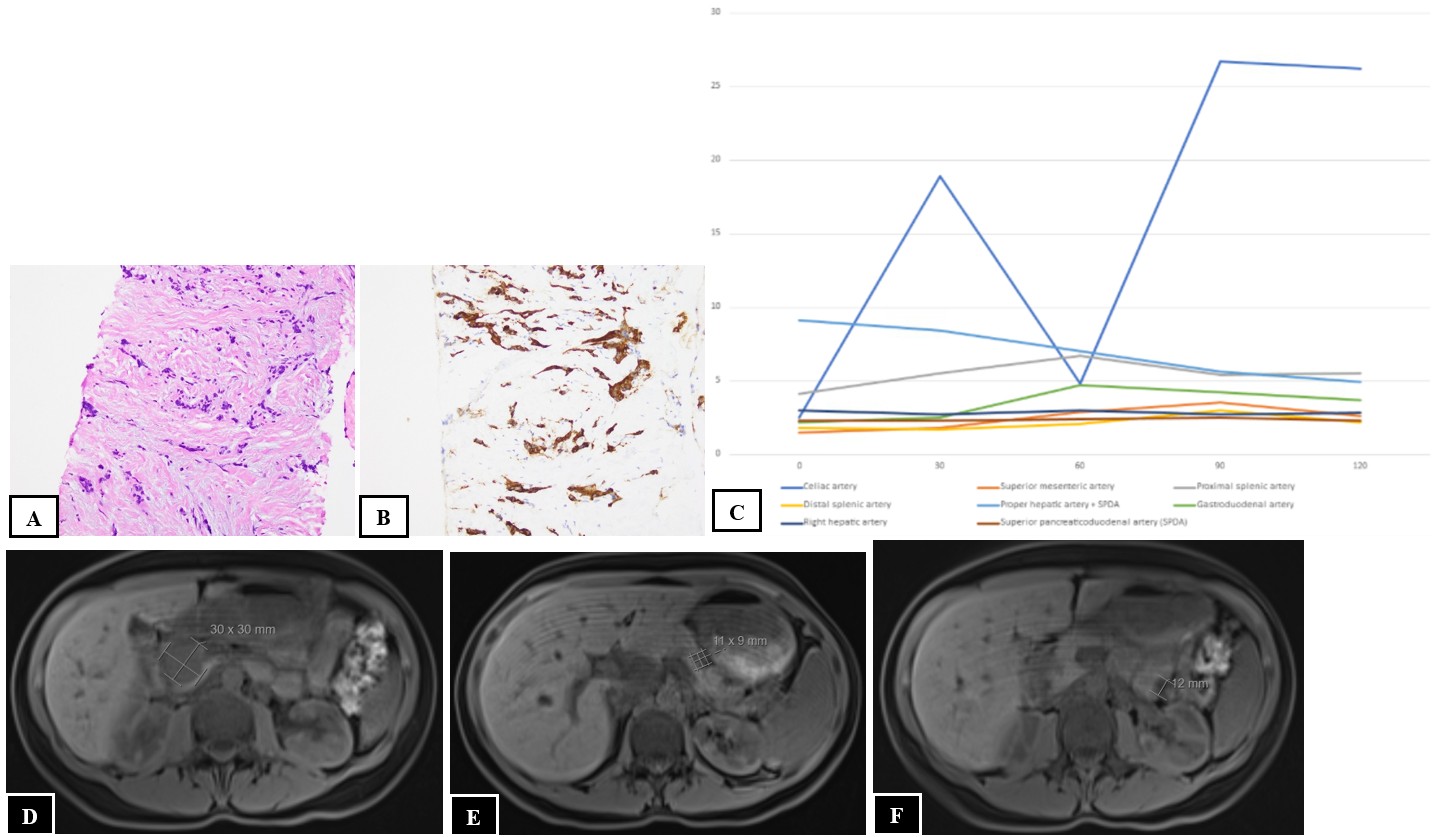
A 41-year-old female with multiple endocrine neoplasia type 1 presented with a 10-year history of recurrent fasting hypoglycemia. Fasting labs revealed blood glucose 54 mg/dL, insulin 3.8 mIU/L, proinsulin 9.8 pmol/L, and C-peptide 1.8 ng/mL. CT abdomen/pelvis demonstrated a large 2.4 x 2.5 x 2.9 cm well-circumscribed pancreatic head mass and three pancreatic body and tail lesions (Figures 1A-D). Dotatate PET/CT revealed a somatostatin avid pancreatic head mass, pancreatic tail nodules, and multiple hepatic, retroperitoneal, and peripancreatic lesions consistent with metastatic insulinoma (Figures 1E-F). EUS revealed a 31 mm x 27 mm pancreatic head mass, 12 mm pancreatic tail lesion, and sub-centimeter left hepatic lesion (Figures 1G-I). Fine needle aspiration of the pancreatic head mass confirmed well-differentiated NET (Figures 2A-B). A selective arterial calcium stimulation test (SACST) identified the source of pathologic insulin production in the pancreatic body/tail despite the dominant lesion in the head (Figure 2C). She underwent EUS-RFA with five ablations of an 11 mm lesion in the pancreatic body for 11-18 seconds, five ablations of an 11 mm lesion in the pancreatic tail for 15-22 seconds, and two ablations of an 8 mm lesion in the pancreatic tail for 16-17 seconds using a 10 mm trocar. One day after EUS-RFA, fasting labs revealed blood glucose 117 mg/dL, insulin 4.8 mIU/L, C-peptide 2.6 ng/mL, and she reported no episodes of hypoglycemia at follow-up. Two months after EUS-RFA, MRI abdomen/pelvis demonstrated small pancreatic body and tail lesions without enhancement at sites of ablation and unchanged pancreatic head mass and hepatic, retroperitoneal, and peripancreatic lesions (Figures 2D-F).
In a patient with metastatic insulinoma, the SACST was successful in localizing the source of pathologic insulin production to guide treatment with EUS-RFA. Despite limited reports of EUS-RFA for insulinomas and none in the setting of metastatic disease, this modality appears to be a promising potential approach, in this case guided by the SACST to target sites of disease.