P1147 - Efficacy of Guselkumab in Moderately to Severely Active Ulcerative Colitis by Extent of Disease and Inflammatory Burden: Subgroup Analysis of the Phase 3 QUASAR Maintenance Study
Division of Gastroenterology, Hepatology, and Endoscopy, Brigham and Women’s Hospital, Harvard Medical School Boston, MA
Award: ACG Presidential Poster Award
Jessica R.. Allegretti, MD, MPH1, Tadakazu Hisamatsu, MD, PhD2, Brian Bressler, MD, MS3, Laurent Peyrin-Biroulet, MD, PhD4, Matthew Germinaro, MD5, Shadi Yarandi, MD5, Nicole Shipitofsky, PharmD5, Ye Miao, MS5, Bruce E. Sands, MD, MS, FACG6, David T. Rubin, MD7, Axel Dignass, MD, PhD8 1Division of Gastroenterology, Hepatology, and Endoscopy, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA; 2Department of Gastroenterology and Hepatology, Kyorin University School of Medicine, Tokyo, Tokyo, Japan; 3University of British Columbia, Vancouver, BC, Canada; 4Department of Gastroenterology, CHRU Nancy, INSERM NGERE, Université de Lorraine, France, Vandœuvre-lès-Nancy, Lorraine, France; 5Johnson & Johnson, Spring House, PA; 6Dr. Henry D. Janowitz Division of Gastroenterology, Icahn School of Medicine at Mount Sinai, New York, NY, USA, New York, NY; 7University of Chicago Medicine Inflammatory Bowel Disease Center, Chicago, IL, USA, Chicago, IL; 8Agaplesion Markus Hospital, Frankfurt, Hessen, Germany
Introduction: Guselkumab (GUS) is a dual-acting IL-23 inhibitor.1 In the Phase 3 QUASAR maintenance study (NCT04033445), both the GUS 100mg every 8 weeks (q8w) and 200mg q4w subcutaneous (SC) maintenance dose regimens were efficacious.2 Here, we evaluated efficacy of these dose regimens in clinically relevant subgroups of participants (pts) with and without extensive ulcerative colitis (UC) disease or high inflammatory burden.
Methods: Clinical responders after 12 weeks of GUS intravenous (IV) induction were randomized 1:1:1 to GUS 100mg SC q8w, GUS 200mg SC q4w or placebo (PBO) (GUS withdrawal) at start of the maintenance study (M-0). Efficacy endpoints were analyzed at Week (W)44 in the primary analysis population of pts randomized and treated in the maintenance study who had a modified Mayo score of 5-9 at induction baseline (I-0). Subgroup analyses were conducted by (1) extent of UC disease (limited to left side of colon vs extensive) based on screening endoscopy and/or medical history at I-0 and (2) inflammatory burden based on serum C-reactive protein (CRP) levels (≤3 vs >3mg/L) at M-0.
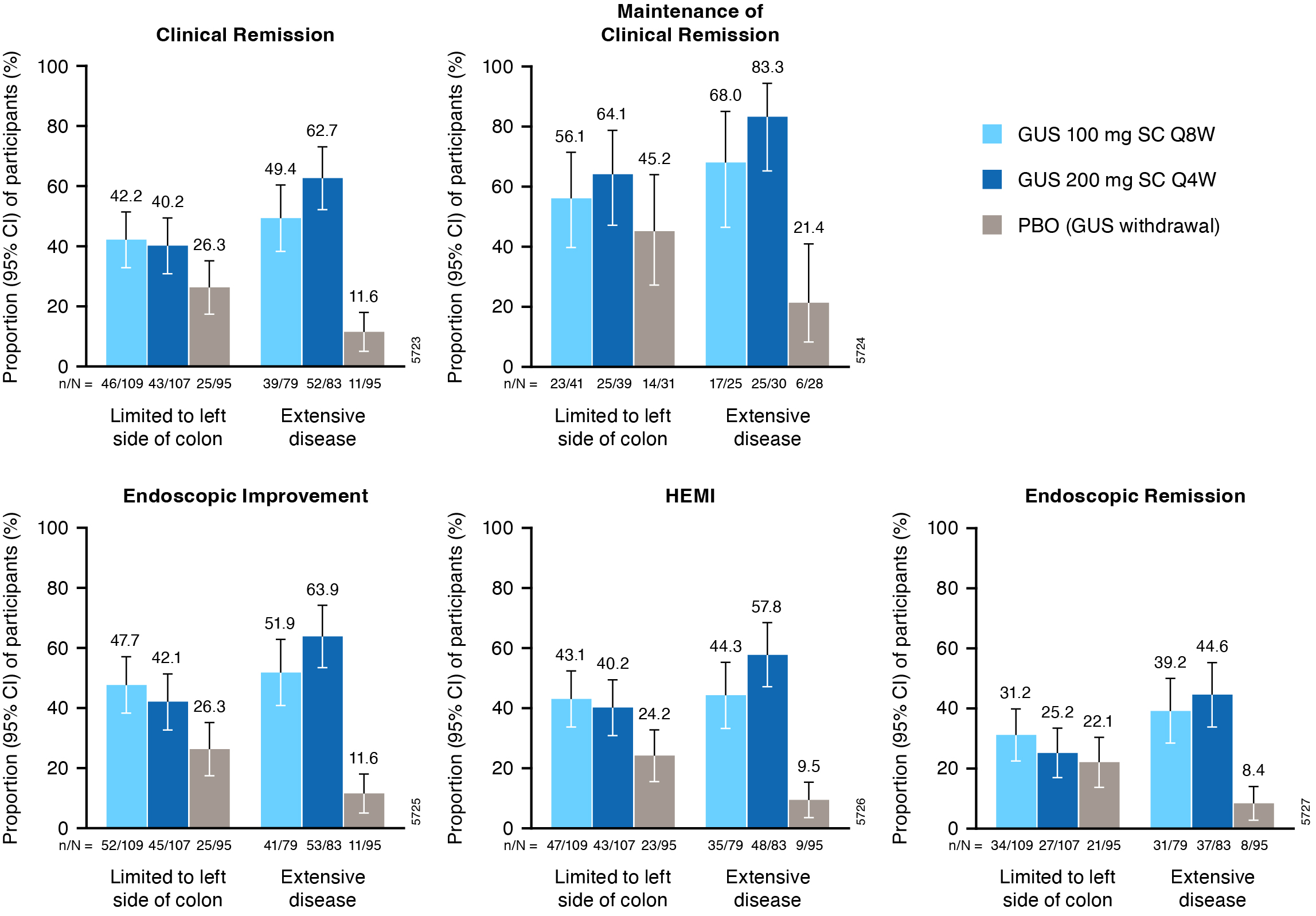
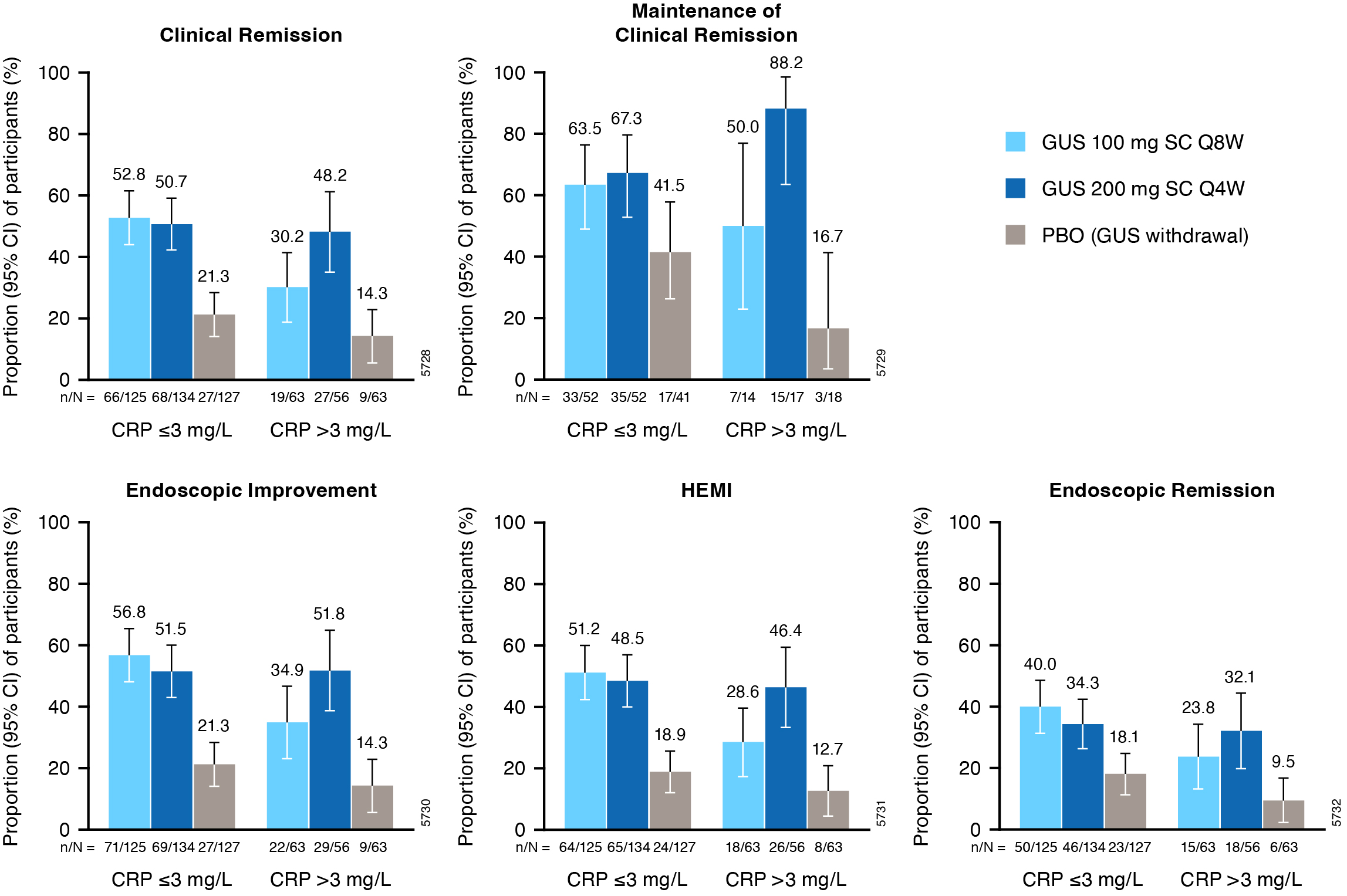
Results: Of 568 pts in the primary analysis population, 257 (45.2%) had extensive UC disease at I-0 and 182 (32.0%) had serum CRP >3mg/L at M-0. Proportions of pts achieving W44 clinical and histologic-endoscopic efficacy endpoints were greater with both GUS dose regimens vs PBO across subgroups (Figures). For pts with extensive UC disease, the proportion of pts achieving clinical remission at W44 was numerically greater with GUS 200mg q4w (62.7%) relative to GUS 100mg q8w (49.4%) (PBO, 11.6%). For those with elevated CRP ( >3mg/L) at M-0, clinical remission at W44 was achieved by 48.2% of GUS 200mg q4w vs 30.2% of GUS 100mg q8w pts (PBO, 14.3%). Proportions of pts achieving endoscopic improvement, histo-endoscopic improvement, endoscopic remission, and maintenance of clinical remission were also greater with GUS 200mg q4w in these subgroups. Among pts with disease limited to the left side of the colon or CRP ≤3mg/L at M-0, proportions of pts achieving these efficacy endpoints were similar with GUS 100mg q8w and GUS 200mg q4w.
Discussion: For pts with moderately to severely active UC with extensive disease or high inflammatory burden, greater efficacy rates were observed with GUS 200mg SC q4w compared with GUS 100mg SC q8w.
References: 1. Sachen KL et al. Front Immunol 2025;16:1532852; 2. Rubin DT et al. Lancet 2025;405:33-49.
Figure: Figure 1. Key efficacy endpoints at maintenance W44 in subgroups of pts from QUASAR defined by extent of UC disease (limited to left side of colon vs extensive) at induction baseline. Includes pts with modified Mayo score of 5-9 at induction baseline who achieved clinical response to GUS induction and were re randomized at maintenance study entry. Error bars represent 95% CIs for proportions of pts meeting the endpoint in each group based on the normal approximation confidence limits, except for maintenance of clinical remission where CIs were based on the exact confidence limits. Clinical remission is defined as a stool frequency subscore of 0 or 1 and not increased from induction baseline, a rectal bleeding subscore of 0, and an endoscopy subscore of 0 or 1 with no friability. Maintenance of clinical remission is defined as clinical remission at W44 among pts in clinical remission at maintenance baseline (denominator is pts with clinical remission at maintenance baseline). Endoscopic improvement is defined as an endoscopy subscore of 0 or 1 with no friability. HEMI is defined as achieving a combination of histologic improvement and endoscopic improvement. Endoscopic remission is defined as an endoscopy subscore of 0. Pts who had an ostomy or colectomy, dose adjustment, prohibited change in UC medication, or who discontinued study agent due to lack of efficacy or an AE of worsening of UC prior to W44 were considered not to have achieved the efficacy endpoints. For pts who discontinued study agent due to COVID-19 related reasons (excluding COVID-19 infection) or regional crisis in Russia and Ukraine prior to W44, the observed values were used if available. Pts who discontinued study agent for other reasons prior to W44 were considered not to have achieved the endpoint. Nonresponder imputation for missing data: pts who were missing one or more of the components pertaining to an endpoint at W44 were considered not to have achieved the endpoint. Pts who had an unevaluable biopsy were considered not to have achieved histologic endpoints. AE=Adverse event; CI=Confidence interval; GUS=Guselkumab; HEMI=Histologic-endoscopic mucosal improvement; PBO=Placebo; pts=Participants; Q4W=Every 4 weeks; Q8W=Every 8 weeks; SC=Subcutaneous; UC=Ulcerative colitis; W=Week.
Figure: Figure 2. Key efficacy endpoints at maintenance W44 in subgroups of pts defined by inflammatory burden (serum CRP ≤3 vs >3mg/L) at maintenance study baseline. Includes pts with modified Mayo score of 5-9 at induction baseline who achieved clinical response to GUS induction and were re randomized at maintenance study entry. Error bars represent 95% CIs for proportions of pts meeting the endpoint in each group based on the normal approximation confidence limits, except for maintenance of clinical remission where CIs were based on the exact confidence limits. Clinical remission is defined as a stool frequency subscore of 0 or 1 and not increased from induction baseline, a rectal bleeding subscore of 0, and an endoscopy subscore of 0 or 1 with no friability. Maintenance of clinical remission is defined as clinical remission at W44 among pts in clinical remission at maintenance baseline (denominator is pts with clinical remission at maintenance baseline). Endoscopic improvement is defined as an endoscopy subscore of 0 or 1 with no friability. HEMI is defined as achieving a combination of histologic improvement and endoscopic improvement. Endoscopic remission is defined as an endoscopy subscore of 0. Pts who had an ostomy or colectomy, dose adjustment, prohibited change in UC medication, or who discontinued study agent due to lack of efficacy or an AE of worsening of UC prior to W44 were considered not to have achieved the efficacy endpoints. For pts who discontinued study agent due to COVID-19 related reasons (excluding COVID-19 infection) or regional crisis in Russia and Ukraine prior to W44, the observed values were used if available. Pts who discontinued study agent for other reasons prior to W44 were considered not to have achieved the endpoint. Nonresponder imputation for missing data: pts who were missing one or more of the components pertaining to an endpoint at W44 were considered not to have achieved the endpoint. Pts who had an unevaluable biopsy were considered not to have achieved histologic endpoints. AE=Adverse event; CI=Confidence interval; CRP=C-reactive protein; GUS=Guselkumab; HEMI=Histologic-endoscopic mucosal improvement; PBO=Placebo; pts=Participants; Q4W=Every 4 weeks; Q8W=Every 8 weeks; SC=Subcutaneous; UC=Ulcerative colitis; W=Week.
Axel Dignass: Abbvie – Consultant, fees for participation in clinical trials, review activities such as data monitoring boards, statistical analysis and endpoint committees; manuscripts, Speakers Bureau. Abivax – fees for participation in clinical trials, review activities such as data monitoring boards, statistical analysis and end point committees. Amgen – Consultant. Arena Pharmaceuticals – Consultant. Biogen – Consultant, Speakers Bureau. Boehringer Ingelheim – Consultant. Bristol Myers Squibb – Consultant. CED Service GmbH – Speakers Bureau. Celltrion – Consultant, Speakers Bureau. Dr Falk Foundation – Consultant, fees for participation in clinical trials, review activities such as data monitoring boards, statistical analysis and endpoint committees; manuscripts, Speakers Bureau. Ferring – Consultant, Speakers Bureau. Fresenius Kabi – Consultant. Galapagos – Consultant, fees for participation in clinical trials, review activities such as data monitoring boards, statistical analysis and end point committees, Speakers Bureau. Gilead – fees for participation in clinical trials, review activities such as data monitoring boards, statistical analysis and end point committees, Speakers Bureau. High5MD – Speakers Bureau. Johnson & Johnson – Consultant, fees for participation in clinical trials, review activities such as data monitoring boards, statistical analysis and endpoint committees; manuscripts, Speakers Bureau. Lilly – Consultant. Materia – Speakers Bureau. MedToday – Speakers Bureau. MSD – Consultant, Speakers Bureau. Pfizer – Consultant, fees for participation in clinical trials, review activities such as data monitoring boards, statistical analysis and end point committees, Speakers Bureau. Pharmacosmos – Consultant. Prima – Speakers Bureau. Roche – Consultant. Sandoz – Consultant. Stada – Consultant. Takeda – Consultant, manuscript preparation, Speakers Bureau. Thieme – manuscript preparation. Tilliots – Consultant, Speakers Bureau. UniMed Verlag – manuscript preparation. Vifor Pharma – Consultant, Speakers Bureau.
Jessica R.. Allegretti, MD, MPH1, Tadakazu Hisamatsu, MD, PhD2, Brian Bressler, MD, MS3, Laurent Peyrin-Biroulet, MD, PhD4, Matthew Germinaro, MD5, Shadi Yarandi, MD5, Nicole Shipitofsky, PharmD5, Ye Miao, MS5, Bruce E. Sands, MD, MS, FACG6, David T. Rubin, MD7, Axel Dignass, MD, PhD8. P1147 - Efficacy of Guselkumab in Moderately to Severely Active Ulcerative Colitis by Extent of Disease and Inflammatory Burden: Subgroup Analysis of the Phase 3 QUASAR Maintenance Study, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.