Monday Poster Session
Category: Colon
Faisal Kamal, MD
Sidney Kimmel Medical College at Thomas Jefferson University
Philadelphia, PA
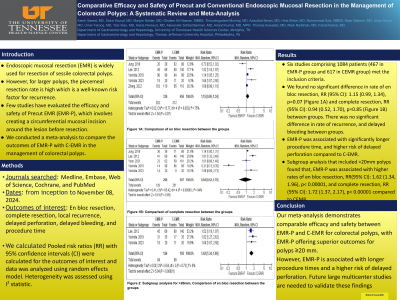
Endoscopic mucosal resection (EMR) is widely used for resection of sessile colorectal polyps. However, for larger polyps, the piecemeal resection rate is high which is a well-known risk factor for recurrence. Few studies have evaluated the efficacy and safety of Precut EMR (EMR-P), which involves creating a circumferential mucosal incision around the lesion before resection. We conducted a meta-analysis to compare the outcomes of EMR-P with C-EMR in the management of colorectal polyps.
Several databases included PubMed, Web of Science, Embase, and the Cochrane were reviewed to identify studies comparing outcomes of EMR-P and CEMR for colorectal polyps from inception to November 08, 2024. Our outcomes of interest were en bloc resection, complete resection, local recurrence, delayed perforation, delayed bleeding, and procedure time. Subgroup analyses were performed for ³20mm polyps. We calculated risk ratios (RRs) with 95% confidence intervals (CIs) for categorical variables and mean differences with 95% CI for continuous variables. Data was analyzed using random effect model. Heterogeneity was assessed using the I2 statistic.
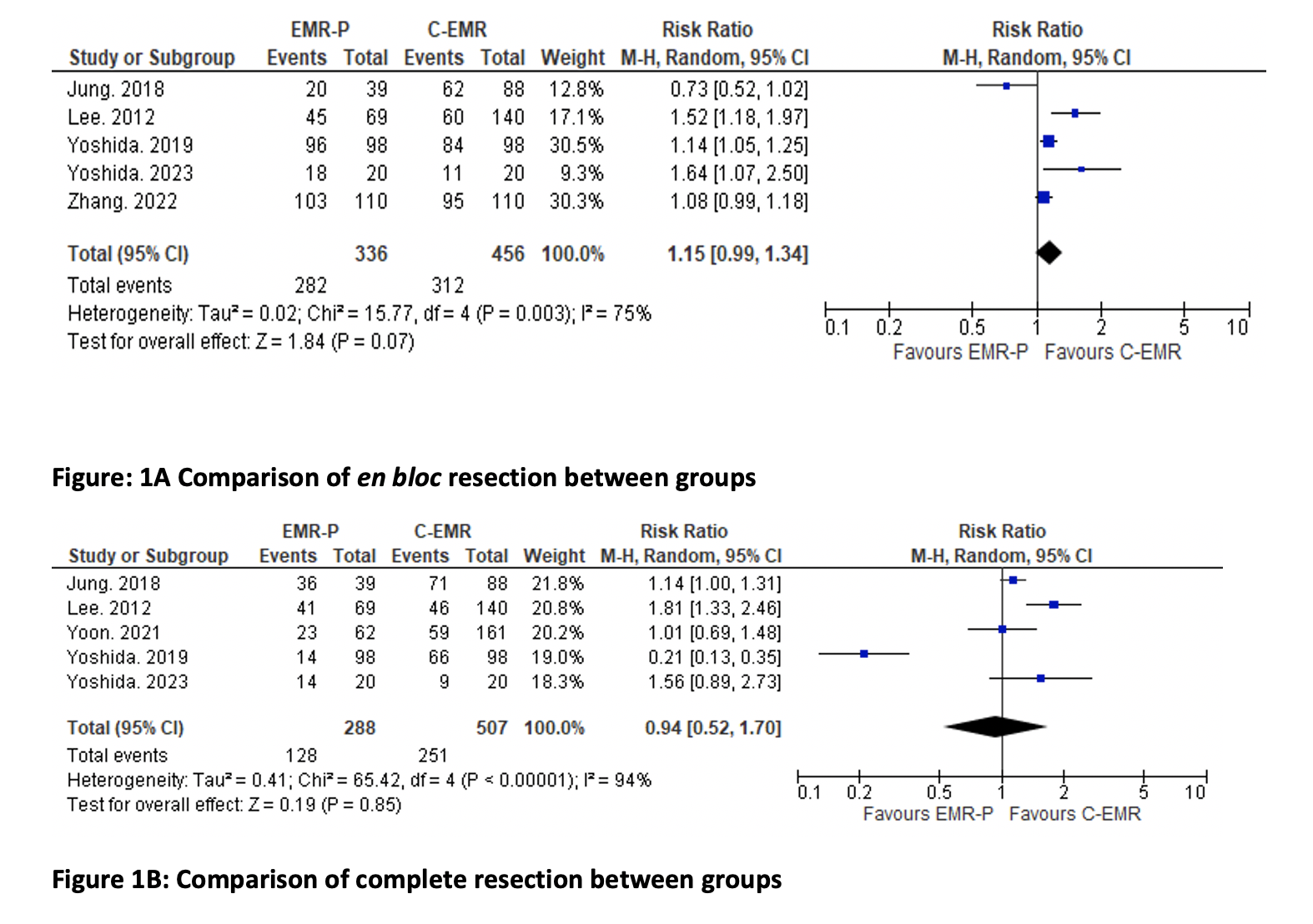
Six studies comprising 1084 patients (467 in EMR-P group and 617 in CEMR group) met the
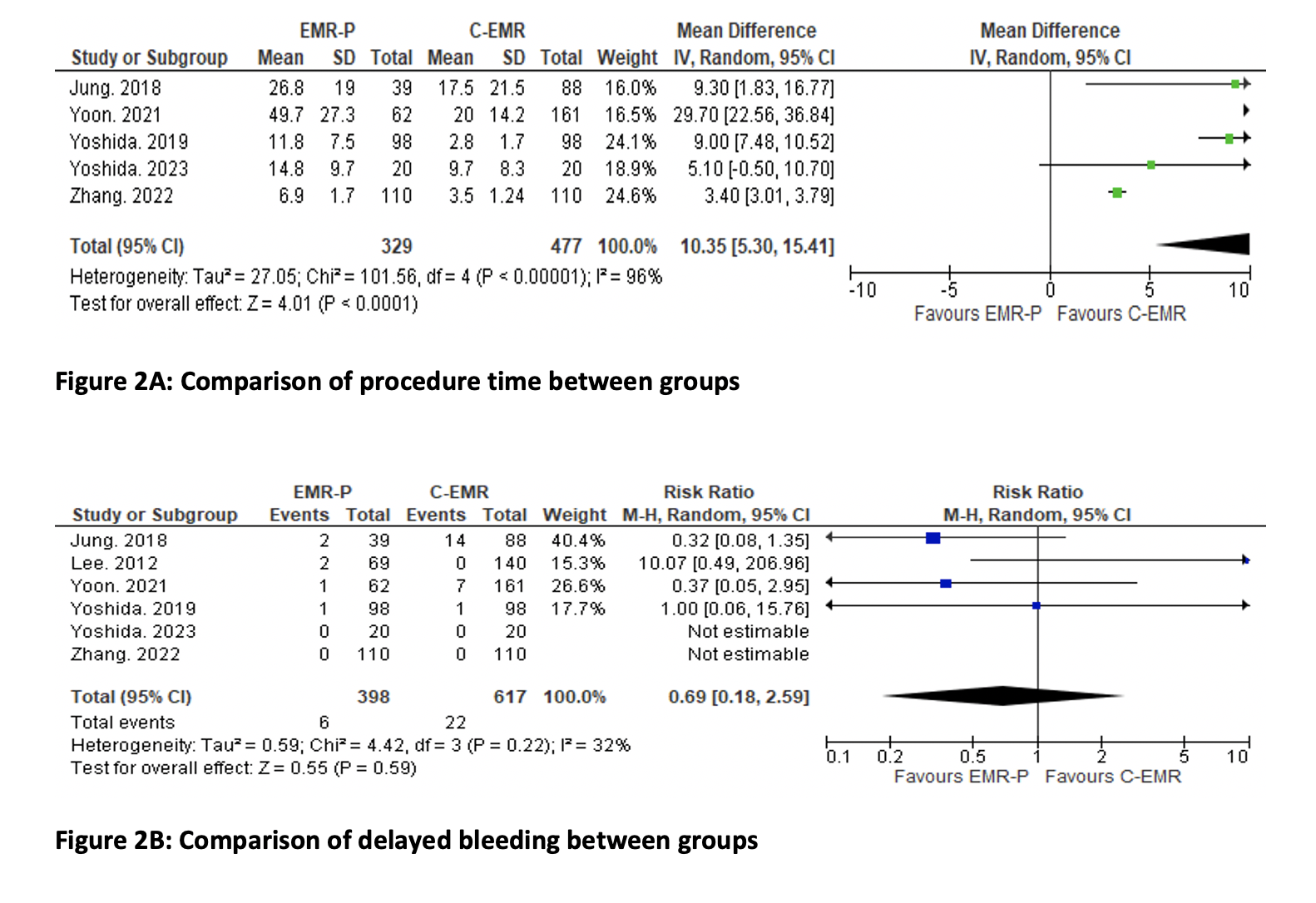
inclusion criteria. We found no significant difference in rate of en bloc resection, RR (95% CI): 1.15 (0.99, 1.34), p=0.07 (Figure 1A) and complete resection, RR (95% CI): 0.94 (0.52, 1.70), p=0.85 (Figure 1B) between groups. There was no significant difference in rate of recurrence, RR (95% CI): 0.35 (0.11, 1.05), p=0.06 and delayed bleeding, RR (95% CI): 0.69 (0.18, 2.59), p=0.59 between groups. EMR-P was associated with significantly longer procedure time, MD (95% CI): 10.35 (5.30, 15.41), p< 0.0001 (Figure 2A) and higher risk of delayed perforation, RR (95% CI): 3.83 (1.35, 10.90), p=0.01 (Figure 2B), compared to C-EMR. Subgroup analysis that included >20mm polyps found that, EMR-P was associated with higher rates of en bloc resection, RR(95% CI): 1.62 (1.34, 1.96), p< 0.00001, and complete resection, RR (95% CI): 1.72 (1.37, 2.17), p< 0.00001 compared to CEMR.
Our meta-analysis demonstrates comparable efficacy and safety between EMR-P and C-EMR for colorectal polyps, with EMR-P offering superior outcomes for polyps ≥20 mm. However, EMR-P is associated with longer procedure times and a higher risk of delayed perforation. Future large multicenter studies are needed to validate these findings