Monday Poster Session
Category: Colon

Shriya Vudari, MD
Louisiana State University
Shreveport, LA
Follicular lymphoma (FL) is a common indolent B-cell non-Hodgkin lymphoma that primarily involves lymph nodes but can occasionally affect extranodal sites. Gastrointestinal (GI) involvement is rare, with the duodenum being the most frequent site. Colonic FL is particularly uncommon and may represent either a primary GI lymphoma or secondary involvement from systemic disease. Herein, we report a rare presentation of a systemic follicular lymphoma diagnosed through colonoscopy.
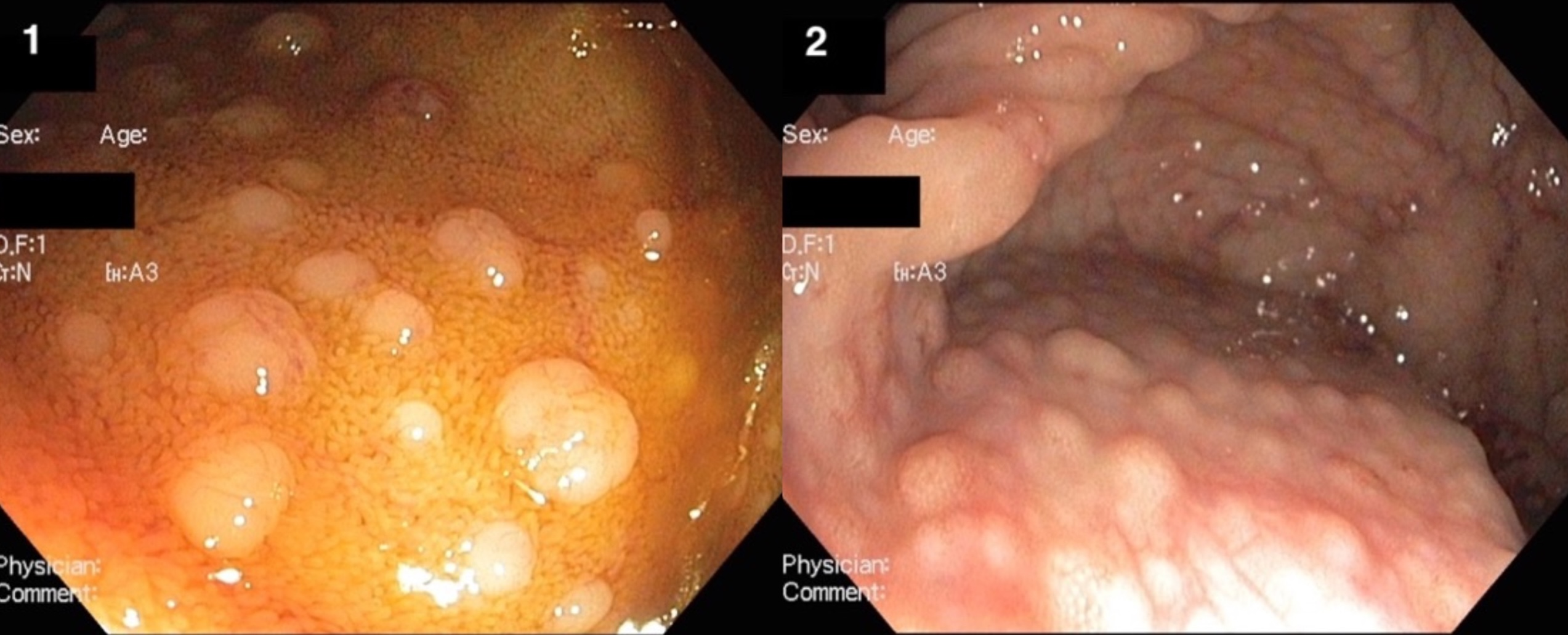
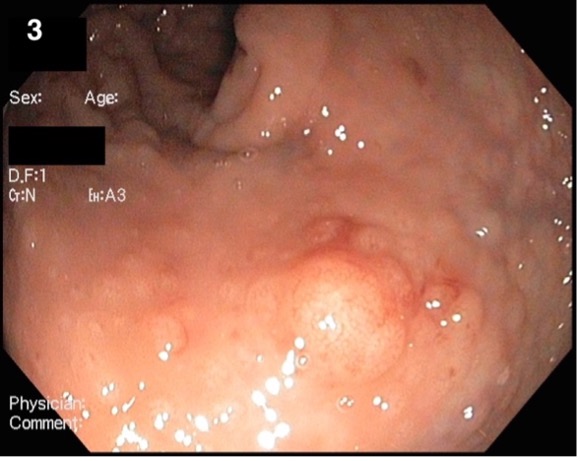
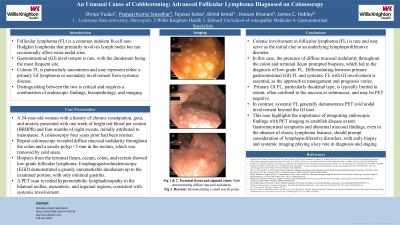
A 54-year-old woman with a medical history of chronic constipation, gout, and anxiety presented with one week of bright red blood per rectum (BRBPR) and a four-month history of night sweats, which she initially attributed to menopause. A colonoscopy performed four years earlier had been normal. Given the new symptoms, the patient underwent a repeat colonoscopy and esophagogastroduodenoscopy (EGD). Colonoscopy revealed diffuse mucosal nodularity throughout the colon and a small sessile polyp (< 5 mm) in the rectum, which was removed by cold snare. The terminal ileum also appeared nodular. EGD showed a grossly unremarkable duodenum up to the examined portion, with only minimal gastritis and no signs of lymphomatous involvement. Multiple biopsies were obtained from the terminal ileum, cecum, colon, and rectum. Histologic examination demonstrated diffuse atypical lymphoid infiltration expanding the lamina propria in a follicular pattern, consistent across all sampled sites. The findings were diagnostic of low-grade follicular lymphoma.
A subsequent PET scan revealed hypermetabolic lymphadenopathy in the bilateral axillary, mesenteric, and inguinal regions, consistent with systemic involvement. The patient was referred to oncology for further evaluation and management of systemic follicular lymphoma with gastrointestinal involvement.
Colonic involvement in follicular lymphoma (FL) is rare and may serve as the initial clue to an underlying lymphoproliferative disorder. Differentiating between primary gastrointestinal (GI) FL and systemic FL with GI involvement is essential, as the approach to management and prognosis varies. Primary GI FL, particularly duodenal type, is typically limited in extent, often confined to the mucosa or submucosa, and may be PET negative. In contrast, systemic FL generally demonstrates PET avid nodal involvement beyond the GI tract. This case highlights the importance of integrating endoscopic findings with PET imaging to establish disease extent.