Monday Poster Session
Category: Colon
.jpg "Madhav Patel, DO photo")
Madhav Patel, DO
University of Chicago Northshore Internal Medicine
Evanston, IL
Extrapulmonary manifestations of mycobacterium tuberculosis are uncommon and difficult to recognize. We present a unique case of a large colonic mass with findings suggestive of peritoneal carcinomatosis, with work up demonstrating colonic TB. Colonic TB can present in a variety of ways and a heightened suspicion should be kept in the differential for an intestinal mass negative for neoplasm or malignancy, especially in those with risk factors for infection.
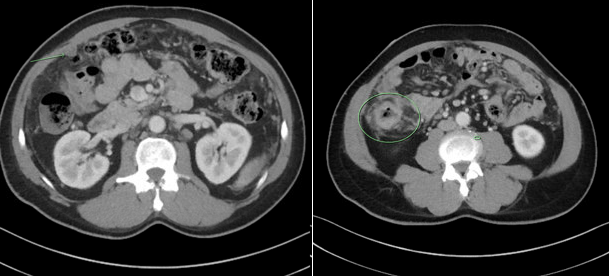
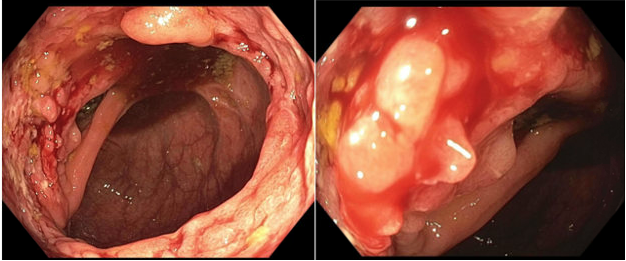
A 52-year old Filipino male with a PMH of CAD, HTN, and HLD presented with hemoptysis and pleuritic pain. He was found to have RLL infiltrates on CT and was admitted for CAP. CT chest was also notable for soft tissue nodularity in the upper abdomen, with concern for carcinomatosis. A CT abdomen/pelvis with contrast revealed intra-abdominal LAD and peritoneal carcinomatosis concerning gastrointestinal malignancy. Colonoscopy was performed with findings of a frond-like villous, ulcerated lesion in the ascending colon. Pinch biopsies were performed and showed severe extensive ulceration and granulation tissue, granulomas, and focal calcifications without dysplasia or malignancy. IHS was positive for CD20 and CD3 but notably GMS and AFB did not reveal any organisms. He was discharged after treatment of pneumonia but was lost to follow-up until 3 months later, when he returned with worsening hemoptysis. Imaging showed progression of his pulmonary nodules with concern for necrotic pneumonia. BAL revealed negative AFB and fungal smear but TB DNA was positive. RIPE therapy was initiated and follow-up examination revealed symptom improvement.
Colonic TB remains a rare extrapulmonary manifestation of TB, high suspicion should be maintained in those with risk factors. Extrapulmonary TB presents with several barriers to diagnosis. Serial AFB smears are the mainstay, but they demonstrate a limited sensitivity in pulmonary/ extrapulmonary TB with 22-43% and 0-42% respectively. The positivity rate in colonic TB is approximately 5%. Conversely, TB DNA has demonstrated a sensitivity of 74.9-87.6% and of 9.5-81.6% in pulmonary/extrapulmonary TB respectively, with a 99.7% specificity. Classically, TB in the GI tract presents on CT imaging as nonspecific mural thickening with adjacent fat-stranding and lymphadenopathy. However, when differentiating peritoneal TB from peritoneal carcinomatosis, the omental ring sign and omental thickening has demonstrated a 85% sensitivity and 96% specificity in differentiating the two.