University of Florida Health Shands Hospital Gainesville, FL
Mary Alexandra Bramlage, MD, Nimy John, MD University of Florida Health Shands Hospital, Gainesville, FL
Introduction: Primary gastric lymphoma is uncommon, with an incidence of approximately 2.97 per 100,000 persons per year. Diffuse large B-cell lymphoma (DLBCL) is the most common histologic subtype of primary gastric lymphoma; however, the germinal center B-cell (GCB) phenotype is less frequently found in the stomach (one-third of cases) compared to the activated B-cell (ABC) phenotype.1,2
Case Description/Methods: A 75-year-old male with atrial fibrillation on Eliquis and chronic iron deficiency anemia was admitted to the hospital for abdominal pain, coffee ground emesis, and melena. His baseline hemoglobin was 11 and was found to be 7 on arrival. A CT scan of the abdomen was unremarkable.
He had an EGD and colonoscopy 21 months prior to work up his iron deficiency anemia, which were relatively unremarkable aside from erythematous gastric mucosa. Pathology was diagnostic of Helicobacter pylori (H. pylori), which was treated successfully. Eradication was verified with an H. pylori breath test.
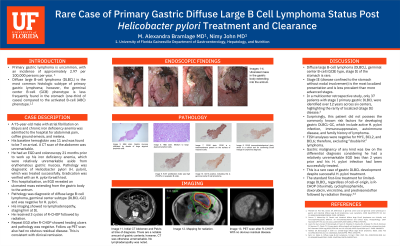
This hospitalization, an EGD revealed an ulcerated mass extending from the gastric body to the antrum. Pathology was diagnostic of diffuse large B-cell lymphoma, germinal center subtype (DLBCL-GC) and was negative for H. pylori. His imaging showed no lymphadenopathy, staging him at IE. His oncology team is planning for 3 cycles of R-CHOP followed by radiation.
Discussion: Diffuse large B-cell lymphoma (DLBCL), germinal center B-cell (GCB) type, stage IE of the stomach is rare. Stage IE (disease confined to the stomach without nodal involvement) is the most localized presentation and is less prevalent than more advanced stages. In a multicenter retrospective study, only 37 patients with stage I primary gastric DLBCL were identified over 12 years across six centers, highlighting the rarity of localized (stage IE) disease.3
Surprisingly, this patient did not possess the commonly known risk factors for developing gastric DLBCL-GC, which include active H. pylori infection, immunosuppression, autoimmune disease, and family history of lymphoma. Additional workup is ongoing, including FISH analyses for MYC with reflex to BCL2 to exclude “double hit” lymphoma.
Gastric malignancy of any kind was low on the differential diagnosis considering he had a relatively unremarkable EGD less than 2 years prior and his H. pylori infection had been successfully treated. This is a rare case of gastric DLBCL development despite successful H. pylori treatment.
Figure: ulcerated mass in gastric body extending to antrum
Disclosures:
Mary Alexandra Bramlage indicated no relevant financial relationships.
Nimy John indicated no relevant financial relationships.
Mary Alexandra Bramlage, MD, Nimy John, MD. P6373 - Rare Case of Primary Gastric Diffuse Large B Cell Lymphoma Status Post <i>Helicobacter pylori</i>: Treatment and Clearance, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.