
Tuesday Poster Session
Category: Colon

Susan Kais, MD
University of Cincinnati
Cincinnati, OH
Colorectal cancer (CRC) is the 3rd most commonly diagnosed cancer & the second leading cause of cancer-related deaths worldwide. CRC incidence has stabilized or declined in high-income countries due to screening in individuals aged 45 & older, there has been a concerning rise in younger populations, termed young-onset colorectal cancer (YO-CRC), which refers to cases diagnosed before age 50. By 2030, YO-CRC is projected to comprise 11% of colon cancer & 23% of rectal cancer diagnoses. This trend suggests a strong birth cohort effect, implicating environmental & lifestyle changes as key contributors. This case report highlights the importance of maintaining a high index of suspicion for CRC in younger patients.
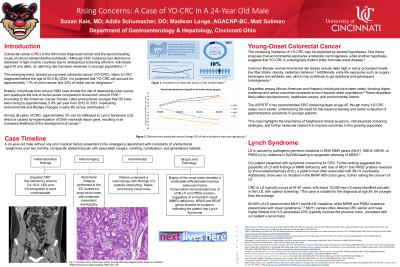
We present a 24-year-old male with no significant PMH who presented to the ED with unintentional weight loss, abdominal pain, nausea, vomiting, constipation, & malaise over 3 months. CT revealed a large cecal mass with extensive mesenteric adenopathy. No family history of CRC. Lab studies showed iron-deficiency anemia & elevated CRP, while tumor markers were unremarkable. Colonoscopy found a partially obstructing cecal mass, & biopsy indicated moderately differentiated invasive adenocarcinoma. Immunostaining revealed loss of MLH1 & PMS2 proteins, suggestive of mismatch repair deficiency. Genetic analysis showed no mutations in NRAS or BRAF, indicating a diagnosis of Lynch Syndrome (LS).
LS, resulting from mutations in DNA mismatch repair genes, typically presents CRC at ages 44 to 61. Our patient’s diagnosis at age 24 is notably early. Absence of BRAF mutations & loss of MLH1 & PMS2 support this diagnosis. Emerging evidence suggests that environmental factors & dietary patterns may contribute to the rising incidence of YO-CRC, including high red meat consumption, low fiber intake, & early-life exposures. Disparities in incidence rates have also been observed among different ethnic groups. The increasing rates of YO-CRC have prompted guideline changes, recommending average-risk screening starting at age 45. However, many YO-CRC patients are diagnosed earlier, necessitating tailored even earlier screening strategies. Our case emphasizes the need for heightened clinical suspicion in young patients presenting with GI symptoms & highlights the importance of earlier diagnostic workup & further research into YO-CRC's molecular mechanisms for improved patient outcomes. As well as the rise of YO-CRC which may again support the need to start CRC earlier than 45.