Tuesday Poster Session
Category: Colon

Ivana Rubenstein, DO
Broward Health Medical Center
Fort Lauderdale, FL
A 55-year-old previously healthy woman presented with acute lower abdominal pain, nausea, vomiting, and hematochezia after returning from a cruise. CT abdomen/pelvis with IV and oral contrast revealed severe colitis in the transverse and descending colon. Colonoscopy confirmed ischemic colitis; biopsies showed acute colitis with focal acute epithelitis. She was treated with IV piperacillin-tazobactam and discharged after clinical improvement.
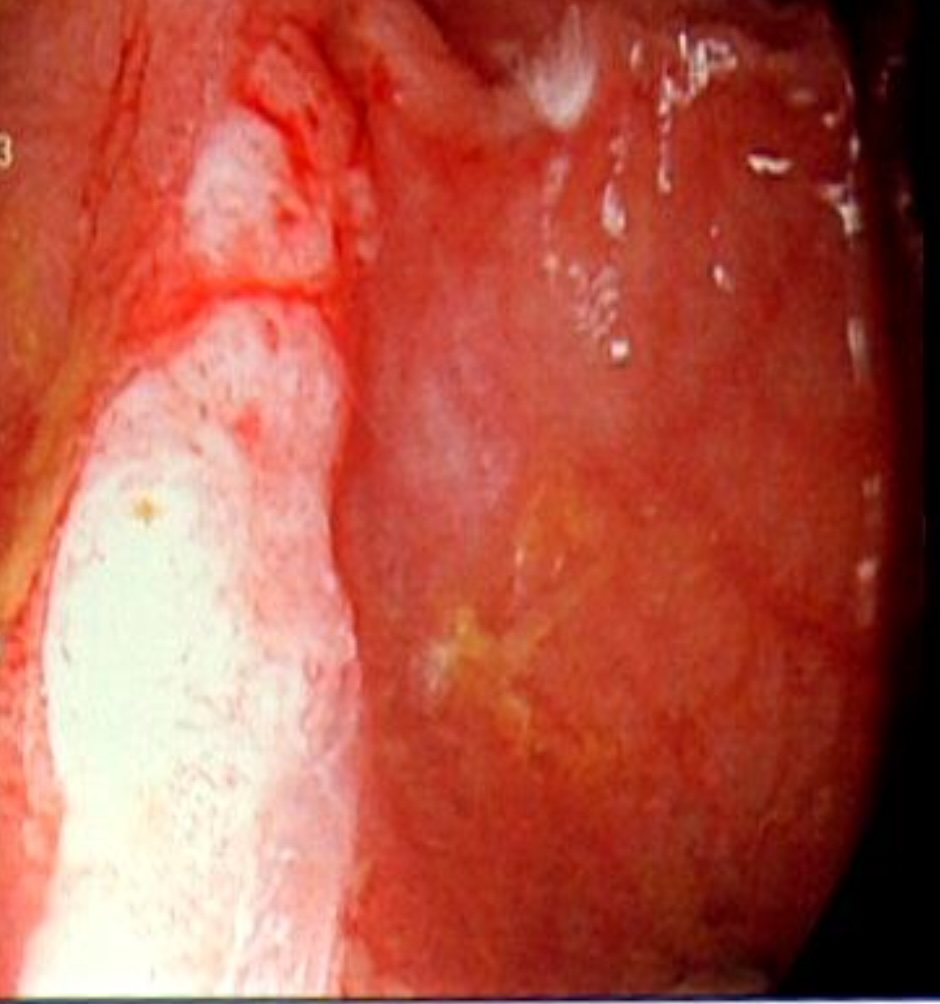
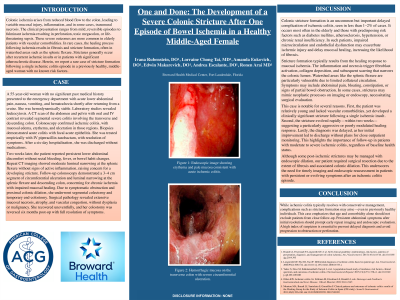
Two weeks later, she developed persistent abdominal pain without bleeding, fever, or constipation. Repeat CT revealed moderate luminal narrowing at the splenic flexure without active inflammation, concerning for a stricture. A follow-up colonoscopy showed a 3–4 cm circumferential ulcerated stricture at the splenic flexure and descending colon. Due to symptom persistence and upstream colonic dilation with fecal impaction, she underwent segmental colectomy with a temporary end-colostomy. Surgical pathology demonstrated mucosal necrosis, atrophy, and vascular congestion consistent with chronic ischemia, with no neoplasia. At three months post-op, she remained symptom-free. Colostomy reversal was successfully performed six months later.