Tuesday Poster Session
Category: Colon
Elizabeth Statham, MD
University of Alabama at Birmingham Hospital
Mountain Brook, AL
Large bowel obstructions (LBOs) account for 20 to 25% of all bowel obstructions and often require urgent surgical intervention. Prompt identification and management of LBO is imperative, particularly as cecal diameter increases to prevent significant morbidity and mortality. LBOs can arise from a multitude of etiologies, most commonly from intrinsic causes such as malignancy or strictures. Extrinsic compression due to fecal impaction represents a rare and atypical etiology of LBO.
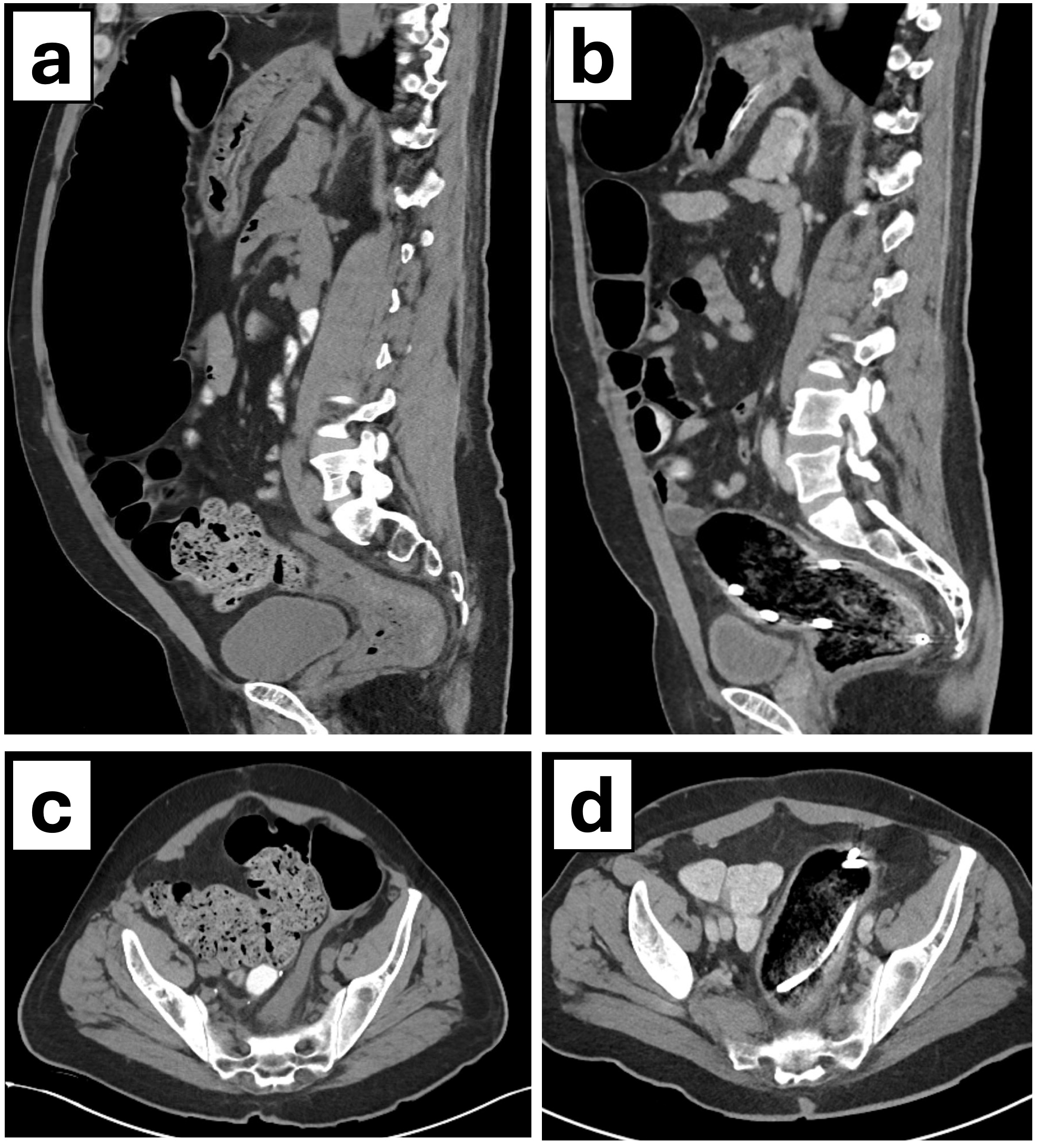
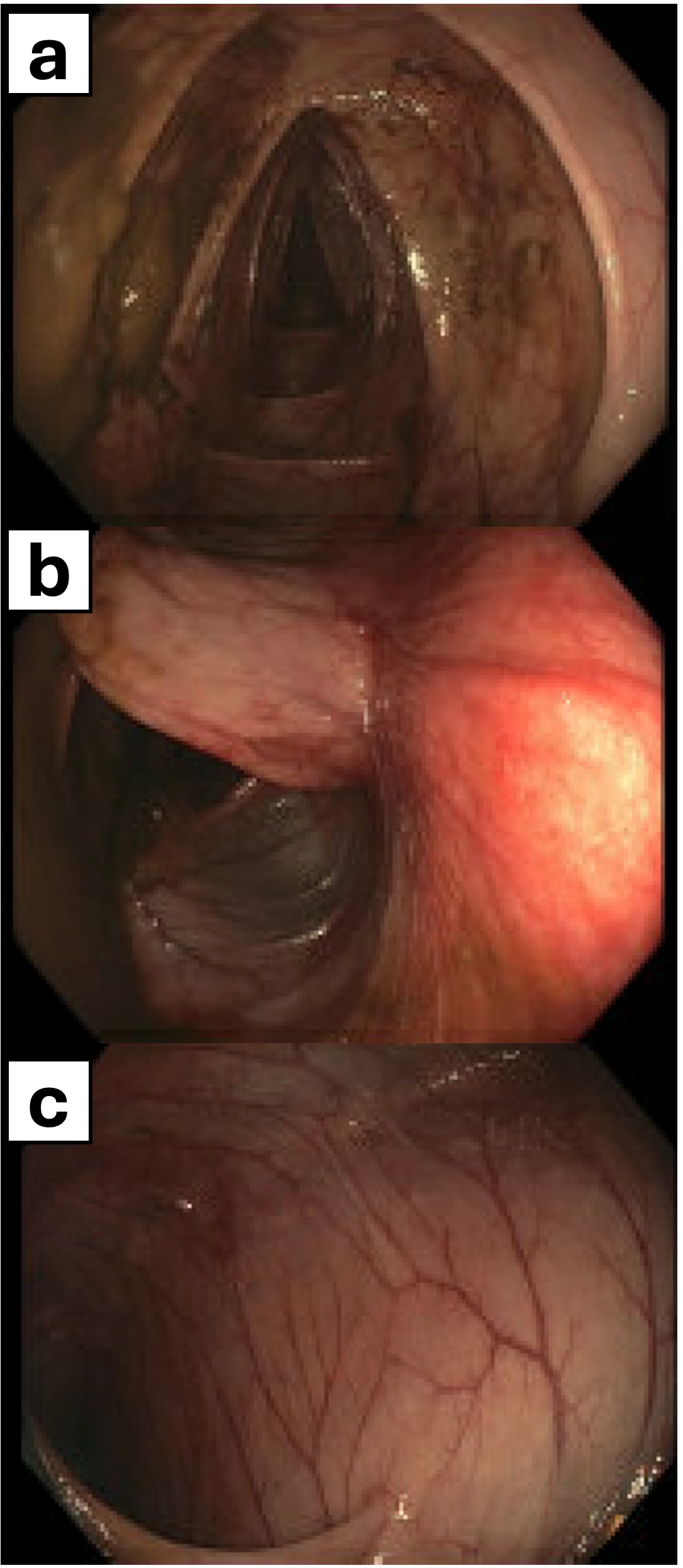
A 55-year-old male with an extensive past surgical history including sigmoid colon resection, ostomy reversal, and ventral hernia repair with mesh was transferred for evaluation of progressive abdominal pain, distension, and nausea. Computed Tomography (CT) imaging showed severe colonic dilatation (Figure 1a, c), most pronounced in the distal transverse colon and descending colon, with the largest segment measuring up to 15.3 cm x 9.6 cm. A transition point was identified distal to patent sigmoidoscopy anastomosis with decompression adjacent to the fecalized cecum and a moderate fecal burden, indicating LBO. CT and endoscopic evaluation (Figure 2) revealed a patent anastomosis, effectively excluding stricture-related obstruction as the cause for LBO. The etiology for LBO was ultimately determined to be due to extrinsic compression from stool burden. Upon endoscopic decompression, the patient experienced symptomatic resolution and reduction in colonic distension confirmed via imaging (Figure 1b, d) without redemonstration of a transition point.
Cases of LBO with cecal diameter exceeding 12 cm incur significantly greater risks, including bowel ischemia, necrosis, and perforation. Although constipation is a common complaint, LBO caused by extrinsic fecal compression-- without mass, stricture, or volvulus-- is exceptionally rare, especially to this degree. This case highlights an unusual presentation LBO in the context of a patent anastomosis, where extrinsic fecal compression resulted in profound colonic dilatation that was successfully managed with endoscopic depression, avoiding surgical intervention. This case underscores the importance of including rare extrinsic causes of LBO in the differential, particularly when imaging reveals colonic dilatation with a patent anastomosis.