Tuesday Poster Session
Category: Colon
.jpg "Amil Shah, DO photo")
Amil Shah, DO
Parkview Medical Center
Pueblo, CO
A 31-year-old male with a history of untreated HIV presented with abdominal pain, unintentional weight loss and occasional night sweats. Initial labs revealed hemoglobin 5.6 g/dL, MCV 84.9 fL, and he received two units of PRBCs. Stool pathogen panel was negative, and fecal calprotectin was not elevated. ESR and CRP were 27 mm/hr and 74 mg/L, respectively. HIV screen showed a positive antibody with a negative p24 antigen. CD4 count was 12 cells/μL, and HIV viral load was 155,000 copies/mL.
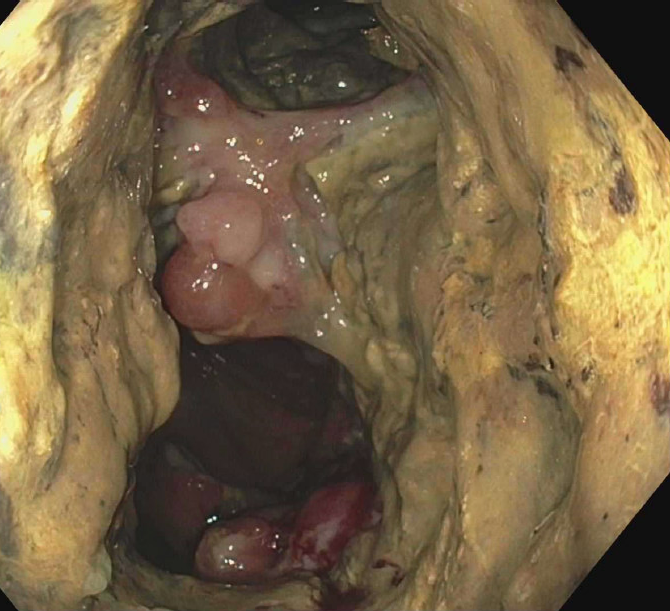
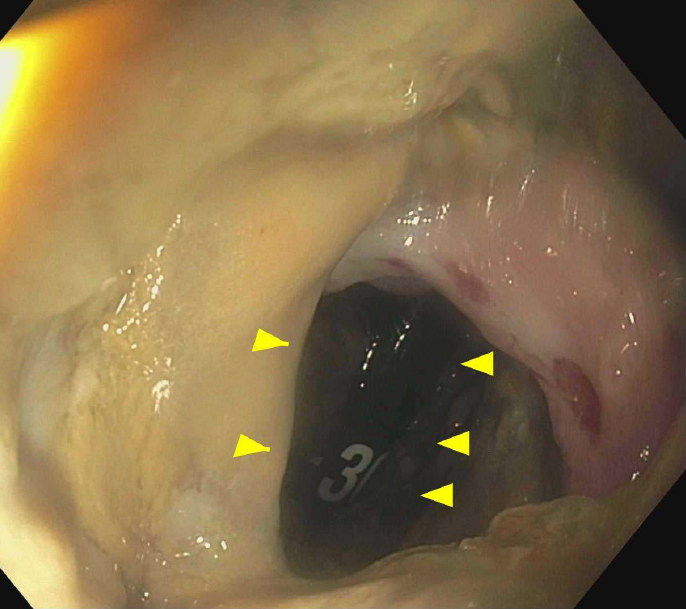
CT abdomen/pelvis showed marked wall thickening of the ascending, hepatic flexure and transverse colon with pericolonic fat stranding. MRI abdomen showed diffuse colitis. Colonoscopy revealed circumferential ulceration and mass-like lesions in the transverse and descending colon, raising concern for colocolonic fistulizing Crohn disease. Biopsies demonstrated high-grade B-cell lymphoma. EGD showed patchy white plaques throughout the esophagus with biopsy confirming esophageal candidiasis.
The patient was empirically started on IV ceftriaxone, metronidazole and fluconazole. HAART was initiated along with trimethoprim-sulfamethoxazole for primary prophylaxis of pneumocystis pneumonia. Due to his immunocompromised state, he was deemed a poor surgical candidate. Oncology was consulted and initiated treatment with R-CHOP. He was discharged with close follow-up plans for chemotherapy and HIV management.