
Tuesday Poster Session
Category: Colon
Joann Ha, DO
Jefferson Health
Voorhees, NJ
A 74-year-old male with a significant past medical history of stage IIIB pancreatic adenocarcinoma, status post distal pancreatectomy and splenectomy with adjuvant chemotherapy and radiation, as well as a history of sigmoid colon cancer, presented with abdominal pain.
He was evaluated by oncology in the outpatient setting after a recent computed tomography (CT) scan demonstrated local progression of his pancreatic cancer. The patient had previously received multiple lines of therapy, including adjuvant capecitabine with gemcitabine, followed by chemoradiation after undergoing a Whipple procedure. A prior PET scan had demonstrated hypermetabolic activity in several locations: the left retroperitoneum (between the adrenal gland and aorta), lower abdominal wall musculature, and sigmoid colon.
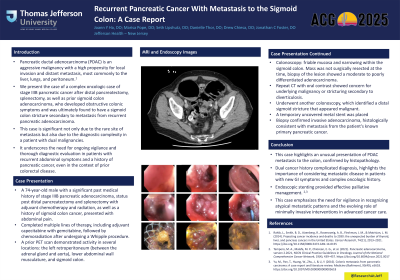
Given these findings, the patient underwent colonoscopy, which revealed friable mucosa and narrowing within the sigmoid colon. Although the mass was not surgically resected at the time, biopsy of the lesion showed a moderate to poorly differentiated adenocarcinoma. A repeat CT with oral contrast again showed persistent sigmoid wall thickening, possibly related to an underlying malignancy or stricturing secondary to diverticulosis. To address the sigmoid obstruction, the patient underwent another colonoscopy, which identified a distal sigmoid stricture that appeared malignant. A temporary uncovered metal stent was placed to relieve the obstruction. Biopsy of the stricture confirmed invasive adenocarcinoma, histologically consistent with metastasis from the patient's known primary pancreatic cancer.