Tuesday Poster Session
Category: Colon

Ahmed Shehadah, MD
United Health Services, Wilson Medical Center
Binghamton, NY
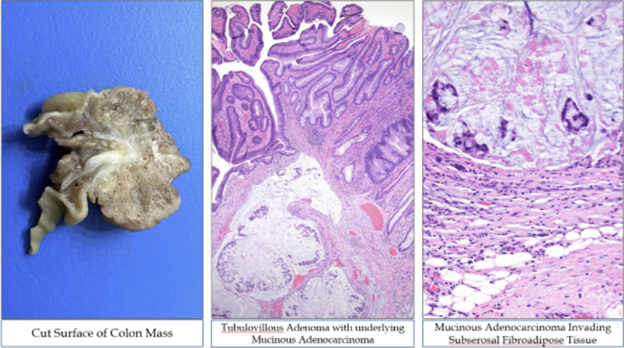
A 27-year-old male with no significant past medical history presented to the emergency room with abdominal pain, nausea, and hematochezia. Vital signs were stable, and laboratory workup, including tumor markers, was unremarkable. Contrast-enhanced computed tomography of the abdomen and pelvis showed a mid-transverse colon intussusception but did not show any mass.
A small bowel follow-through confirmed a partially obstructing intussusception in the transverse colon, and a normal proximal colon. The differential diagnosis included a pathological lead point due to submucosal lymphoid hyperplasia, lipoma, infectious or inflammatory etiologies, malignancy and others.
Colonoscopy was performed to rule out malignancy, and revealed a 46 mm polypoid lesion in the proximal transverse colon, and the area was tattooed for localization. The patient subsequently underwent laparoscopic right colectomy.
Histopathology demonstrated invasive, poorly differentiated mucinous adenocarcinoma of the colon, with invasion into the muscularis propria and subserosal fibroadipose tissue. Resection margins were uninvolved, and all 58 resected lymph nodes were negative. The tumor was classified as stage II mucinous adenocarcinoma. Given the absence of BRAF mutation and MLH1 promoter hypermethylation, genetic germline testing was recommended to evaluate for Lynch syndrome.