P5479 - Mirikizumab Long-Term Impact on Bowel Urgency in Crohn’s Disease and Its Association With Clinical and Other Efficacy Outcomes: Results From the VIVID-2 Open-Label Extension Study
Stephan Vavricka, MD1, David T. Rubin, MD2, Jianmin Wu, 3, Guanglei Yu, PhD4, Aisha Vadhariya, 3, Richard E.. Moses, DO, JD3, Rebecca Hozak, 3, Geert R. D’Haens, MD, PhD5, Simon Travis, 6, Alissa Walsh, MBBS, PhD6 1Department of Gastroenterology and Hepatology, University Hospital Zürich, Zürich, Zurich, Switzerland; 2University of Chicago Medicine Inflammatory Bowel Disease Center, Chicago, IL, USA, Chicago, IL; 3Eli Lilly and Company, Indianapolis, IN; 4Eli Lilly and Company, Indianapolis, Indiana, USA, Indianapolis, IN; 5Department of Gastroenterology, Amsterdam University Medical Center, Amsterdam, Noord-Holland, Netherlands; 6Translational Gastroenterology Unit, University of Oxford and Oxford Biomedical Research Centre, Oxford, UK, Oxford, England, United Kingdom
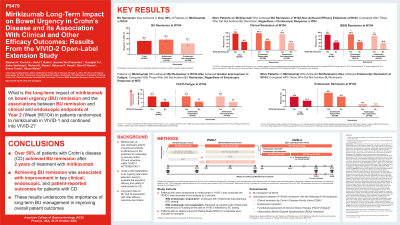
Introduction: Long-term data on bowel urgency (BU) in Crohn’s disease (CD) are limited, and the associations with other efficacy outcomes are not well studied.
Methods: To examine the long-term efficacy of mirikizumab (MIRI) on BU remission and the associations between BU remission and clinical remission, endoscopic remission, and patient-reported outcomes(PRO) improvement at week(W) 104 in patients(pts) with moderately to severely active CD who were randomized to MIRI in the Phase 3 study VIVID-1 and continued into the long-term extension study VIVID-2. In VIVID-1, the MIRI group received induction with 900 mg intravenously (IV) at W0, W4, and W8, then 300 mg subcutaneously (SC) every 4W. W52 endoscopic responders (≥50% reduction from baseline in Simple Endoscopic Score for CD[SES-CD]) continued MIRI SC dosing in VIVID-2. Endoscopic non-responders received reinduction with MIRI IV (3x Q4W) at the start of VIVID-2 followed by SC dosing (IV-SC) as described. Pts having an Urgency Numeric Rating Scale (UNRS) ≥3 at baseline were included in these analyses. BU remission was defined as an UNRS score of ≤2. Associations between BU remission with clinical remission by Crohn’s Disease Activity Index (CDAI), endoscopic remission, Functional Assessment of Chronic Illness Therapy (FACIT)-Fatigue, and Inflammatory Bowel Disease Questionnaire (IBDQ) remission, were assessed at W104, within the VIVID-1 W52 endoscopic response subgroups and the MIRI total group.
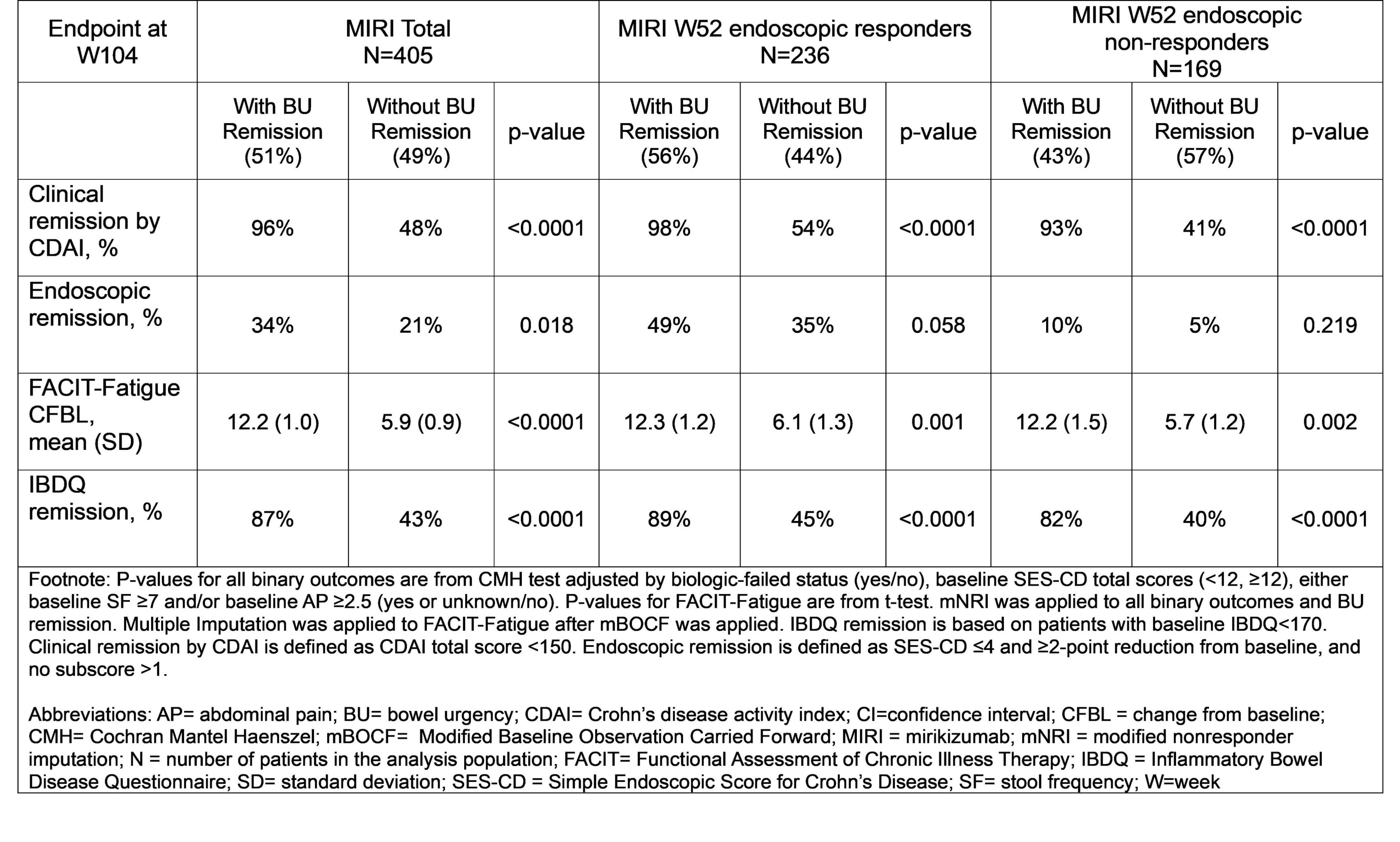
Results: Over 50% of the MIRI total group, 56% MIRI W52 endoscopic responders, and 43% MIRI W52 endoscopic non-responders achieved W104 BU remission. In the MIRI total group, a significantly higher percentage of pts achieved clinical remission, endoscopic remission and IBDQ remission at W104 in the BU remission group vs those without BU remission. The improvement in fatigue by FACIT-Fatigue score was significantly more in the group with BU remission vs those without BU remission (p< 0.0001). In both MIRI W52 endoscopic responders and non-responders, pts who achieved W104 BU remission, vs who did not, achieved significantly higher rates of clinical remission, greater improvements in FACIT-Fatigue, and higher rates of quality of life improvement measured by IBDQ remission (Table).
Discussion: Over 50% pts with CD achieved BU remission at 2 years of MIRI treatment. Achieving BU remission corresponded with improvements to outcomes important to pts with CD, underscoring the importance of long-term management of BU in improving overall pt outcomes.
Figure: Association Between Bowel Urgency Remission and Clinical, Endoscopic, and Patient-reported Outcomes at W104
Stephan Vavricka, MD1, David T. Rubin, MD2, Jianmin Wu, 3, Guanglei Yu, PhD4, Aisha Vadhariya, 3, Richard E.. Moses, DO, JD3, Rebecca Hozak, 3, Geert R. D’Haens, MD, PhD5, Simon Travis, 6, Alissa Walsh, MBBS, PhD6. P5479 - Mirikizumab Long-Term Impact on Bowel Urgency in Crohn’s Disease and Its Association With Clinical and Other Efficacy Outcomes: Results From the VIVID-2 Open-Label Extension Study, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.