NYC Health + Hospitals/South Brooklyn Health Brooklyn, NY
Bishoy Boulus Elkoumes, MD1, Mark Anthony Fallorina, MD1, Sreekari Kedarisetti, MD2, Aleksandr Khudyakov, MD1, Gangacharan Dubey, MD1 1NYC Health + Hospitals/South Brooklyn Health, Brooklyn, NY; 2South Brooklyn Health, Brooklyn, NY
Introduction: Septic shock is a serious and potentially life-threatening condition caused by an infectious disease that requires urgent diagnosis and intervention. This case report investigates the anomaly of septic shock secondary to liver abscess caused by Fusobacterium nucleatum and further complicated by bicytopenia in a patient with well controlled diabetes. It explores the complexity of the diagnosis, treatment and overall management and highlights the need for a collaborative, multidisciplinary approach. This report adds an important information to the existing clinical literature by describing the rarity and highlights the need of considering rare diseases that arise in immunocompromised patients.
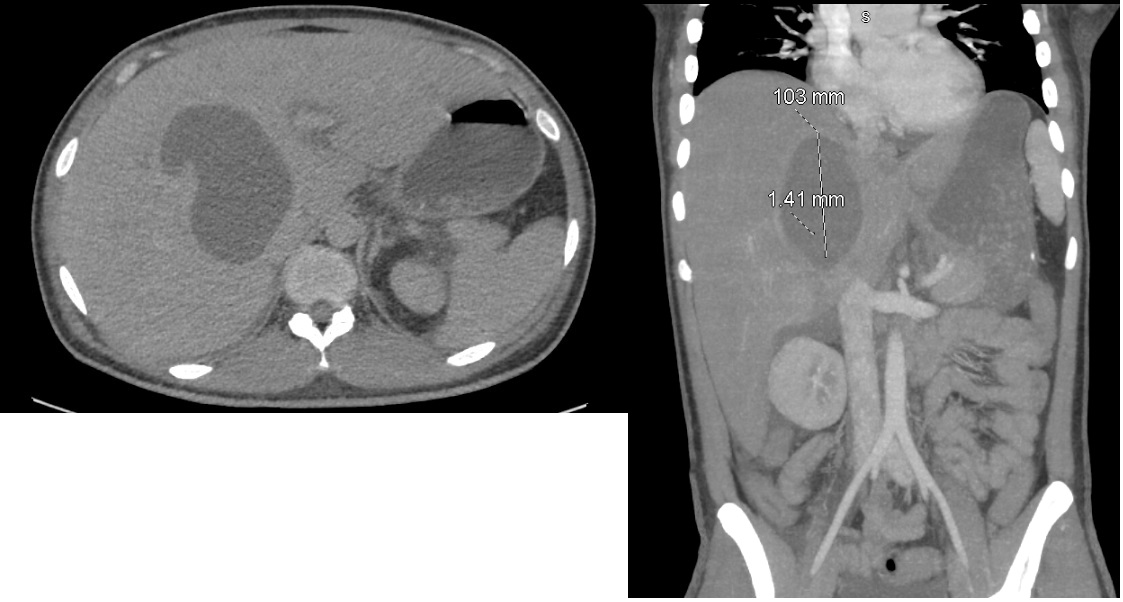
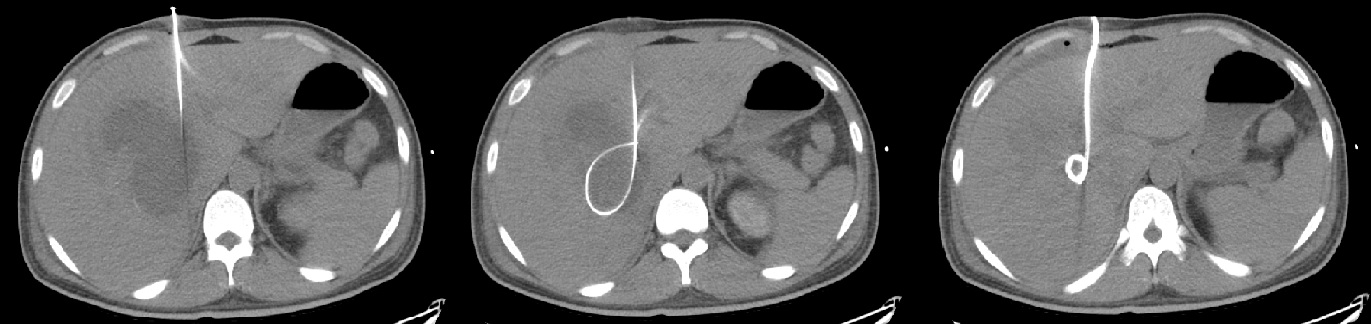
Case Description/Methods: A 25-year-old Asian-American male with controlled type 2 diabetes presented to the emergency department with weakness, malaise, and headache for a few days after returning from Japan. On presentation, he was ill-appearing, febrile, tachycardic, and had abdominal guarding. Labs were notable for leukocytosis, elevated inflammatory markers (CRP, procalcitonin), mild anemia, mild transaminitis, and hyperglycemia. CT scan revealed an enormous bilobed liver abscess (12.8 x 6.1 x 8.8 cm). Patient met the criteria for Septic shock diagnosis, and was treated with broad-spectrum antibiotics, antifungal, fluid resuscitation, and vasopressors. Percutaneous drainage of the liver abscess released 400 mL of purulent material. Gram stain, anaerobic culture of the aspirate and blood cultures revealed F. nucleatum. Antibiotics were de-escalated to piperacillin-tazobactam and metronidazole. The patient then developed bicytopenia, which was secondary to sepsis-associated myelosuppression. With continued antibiotics and glycemic control, the patient improved. Two-month follow-up imaging showed significant resolution of the liver abscess.
Discussion: This case illustrates the complex management of diabetic patients with liver abscesses due to unusual pathogens such as F. nucleatum, an opportunistic anaerobic gram-negative bacillus. Diabetes mellitus makes one susceptible to liver abscesses due to immune compromise and poor glycemic control. The F. nucleatum bacteremia most likely resulted from an occult source, perhaps contracted while he had recently traveled. Effective management of pyogenic liver abscesses involves a multi-disciplinary approach that includes antimicrobial treatment, percutaneous abscess drainage (treatment of choice for large abscesses), and supportive therapy.
Figure: CT Abdomen showing Liver Abscess
Figure: CT Guided Aspiration of Liver Abscess, Drain placement
Disclosures:
Bishoy Boulus Elkoumes indicated no relevant financial relationships.
Mark Anthony Fallorina indicated no relevant financial relationships.
Sreekari Kedarisetti indicated no relevant financial relationships.
Aleksandr Khudyakov indicated no relevant financial relationships.
Gangacharan Dubey indicated no relevant financial relationships.
Bishoy Boulus Elkoumes, MD1, Mark Anthony Fallorina, MD1, Sreekari Kedarisetti, MD2, Aleksandr Khudyakov, MD1, Gangacharan Dubey, MD1. P5632 - A Rare Case of Septic Shock in a Diabetic Patient Secondary to Liver Abscess Caused by <i>Fusobacterium nucleatum</i> Complicated by Pancytopenia, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.