Tuesday Poster Session
Category: Colon


Manasa Ginjupalli, MD
Brooklyn Hospital Center
Brooklyn, NY
We present a 66-year-old male patient with complex medical history, who was initially admitted for hemorrhagic shock caused by a lower gastrointestinal bleed. A colonoscopy was performed, revealing an ulcerated, non-obstructing large mass in the distal rectum, likely the source of the bleeding. However, the biopsy results were non-diagnostic, showing only regular hyperplastic colonic mucosa. The endoscopic images were highly suspicious for an epithelial tumor, likely colorectal cancer, and the patient was advised to undergo an endoscopic ultrasound (EUS) for further evaluation and biopsy of the mass. Unfortunately, he was lost to follow-up.
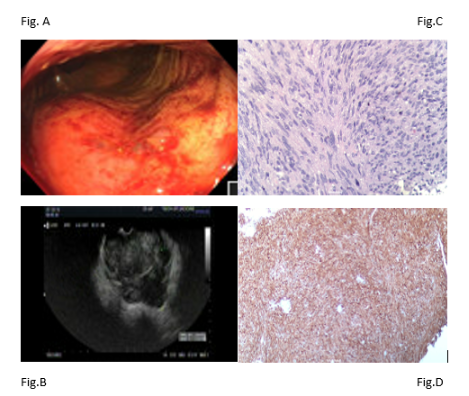
During a subsequent hospital admission for possible ventricular tachycardia, the patient developed another episode of rectal bleeding, likely from the rectal mass. An EUS was performed, which revealed a fungating and ulcerated, non-obstructing large mass in the distal rectum [Fig.A] and fine needle biopsies conducted endo sonographically [Fig.B]. The initial gross findings were suspicious for an epithelial tumor but the surgical pathology revealed a spindle cell neoplasm [Fig.C] , favoring GIST. Immunohistochemical staining was positive for CD117 (c-KIT) [Fig.D], but negative for smooth muscle actin (SMA) and vimentin, confirming the diagnosis.
Given his significant comorbidities, the patient was not considered a surgical candidate. He was referred to oncology, where treatment with imatinib was initiated, and outpatient follow-up was arranged.
GISTs can present in uncommon locations, such as the rectum, and may be challenging to diagnose due to atypical gross findings and non-diagnostic biopsies. It is essential to pursue further evaluation with advanced imaging and immunohistochemistry to ensure an accurate diagnosis and guide appropriate treatment, especially when surgery is not an option.