
Tuesday Poster Session
Category: Colon

Yeshika Thapa, MD
University of Central Florida
Gainesville, FL
Mucinous adenocarcinoma (MAC) accounts for 10–15% of colorectal cancers and is known for its aggressive behavior, higher rates of local invasion, and poor prognosis compared to non-mucinous types. MAC is common in young females, usually presenting in the proximal colon at an advanced stage. Duodenal invasion from right-sided colonic tumors is rare and denotes advanced T4b disease, presenting with vague symptoms of abdominal pain, altered bowel habits, and weight loss.
An 81-year-old male with no prior medical or surgical history presented with an 11 kg weight loss over 10 months, severe abdominal pain radiating to the back, constipation, dark urine, intermittent pruritus with skin discoloration and occasional bloody, foul-smelling stool mixed with mucus.
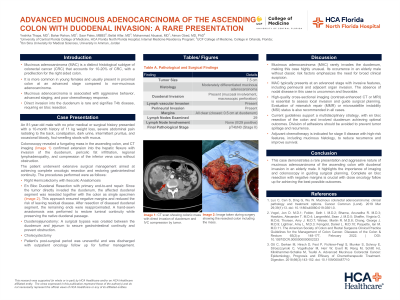
Colonoscopy revealed a fungating mass in the ascending colon. CT imaging confirmed a mass extending to the hepatic flexure with invasion of the duodenum (junction between parts two and three), pericolic fat infiltration, and regional lymphadenopathy without further metastases. The mass also compressed the inferior vena cava, though the patient exhibited no symptoms of venous obstruction.
The patient underwent right hemicolectomy with ileocolic anastomosis, en bloc duodenal resection, primary end-to-end duodenal repair, duodenojejunostomy, and cholecystectomy.
Histopathology showed a 7.5 cm moderately differentiated mucinous adenocarcinoma with duodenal mucosal invasion and macroscopic perforation. Both lymphovascular and perineural invasions were present. All resected margins were clear, with the closest margin (0.5 cm) at the duodenum. All 29 lymph nodes were negative. Additional findings included chronic cholecystitis and fibrofatty obliteration of the appendiceal tip. The final pathological staging was pT4bN0.

