Tuesday Poster Session
Category: Colon
Jessica E. Woodham, DO
University of South Alabama
Mobile, AL
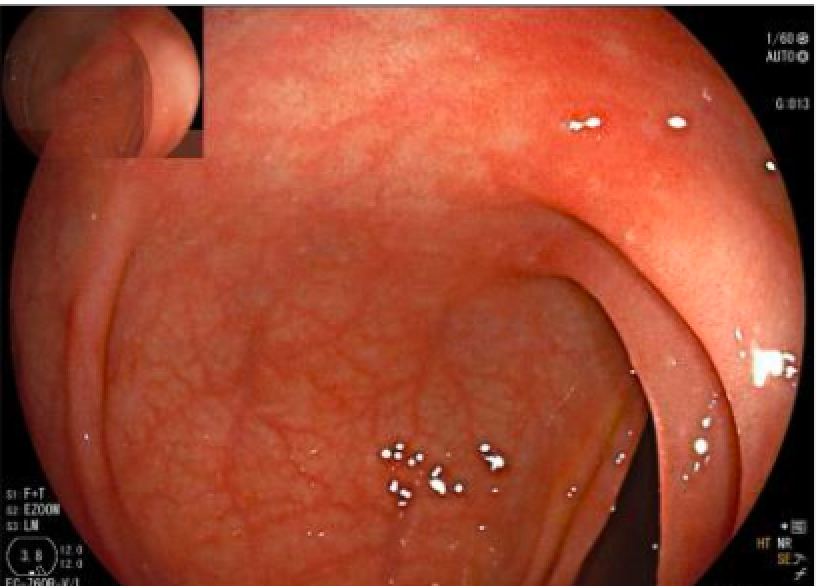
A 61 year old female with invasive ductal carcinoma of the breast was referred to the gastroenterology clinic for evaluation of severe diarrhea. She reported onset of symptoms 3 weeks prior and described watery diarrhea 4 to 5 times per day despite taking loperamide. She denied fever and hematochezia but had some associated abdominal pain and fecal incontinence. She was receiving carboplatin, paclitaxel, and pembrolizumab and last received pembrolizumab one and a half months ago; this regimen was initiated around 3 months prior to presentation. Escitalopram was also started 3 months prior. Infectious stool studies were negative. The patient decided to taper her escitalopram as she did not find it to be efficacious. She was scheduled for a colonoscopy which showed normal terminal ileum but mild patchy colitis in the ascending, transverse, and descending colon. The patient was initiated on controlled ileal release budesonide 9 mg daily. Biopsies revealed lymphocytic colitis throughout the colon. Pembrolizumab was stopped as endoscopic findings were consistent with immune mediated colitis. She noticed rapid improvement in her symptoms after budesonide initiation.