Tuesday Poster Session
Category: Colon
Anum Khakwani, MD
Charleston Area Medical Center
Charleston, WV
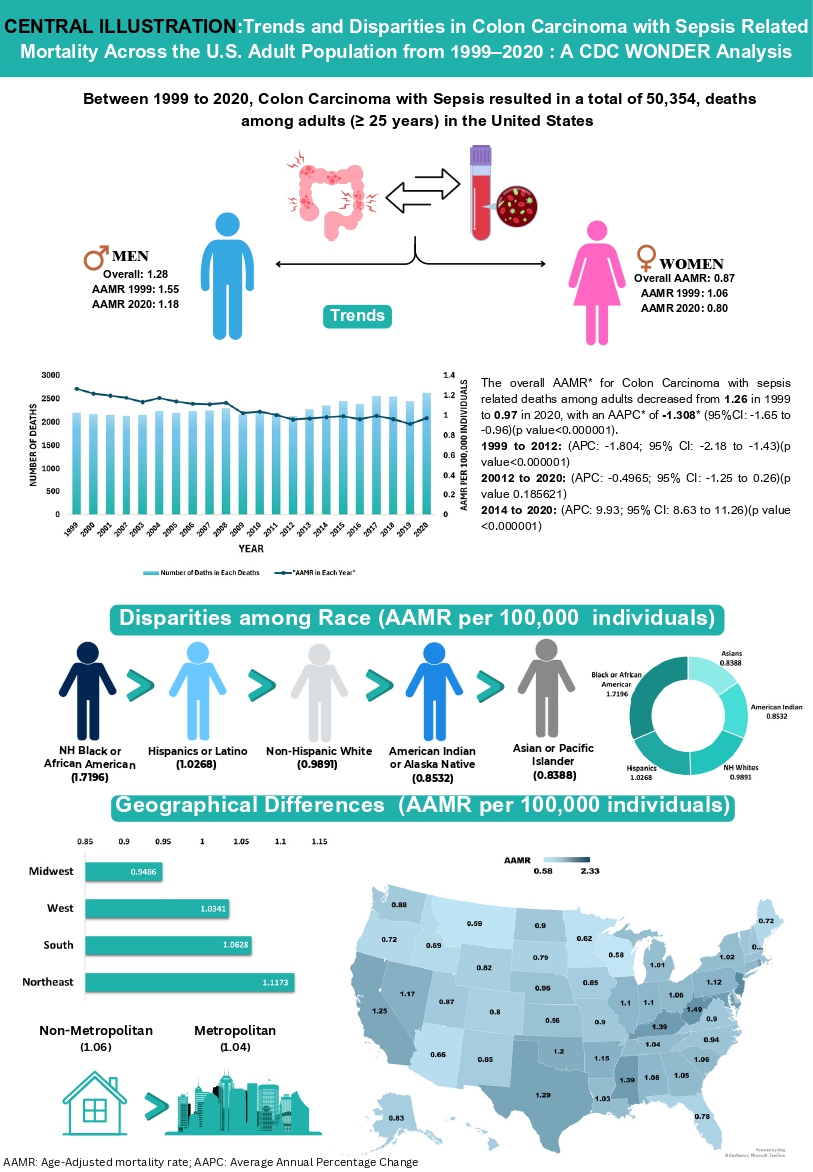
Using CDC WONDER data (1999–2020), we analyzed deaths in adults aged 25+ with ICD-10 codes C18 (colon carcinoma) and A41.9 (sepsis). Age-adjusted mortality rates (AAMRs) per 100,000 were stratified by sex, race/ethnicity, region, state, and urban-rural classification. Joinpoint regression calculated annual percent changes (APCs) and average annual percent changes (AAPCs) with 95% CIs (p< 0.05).
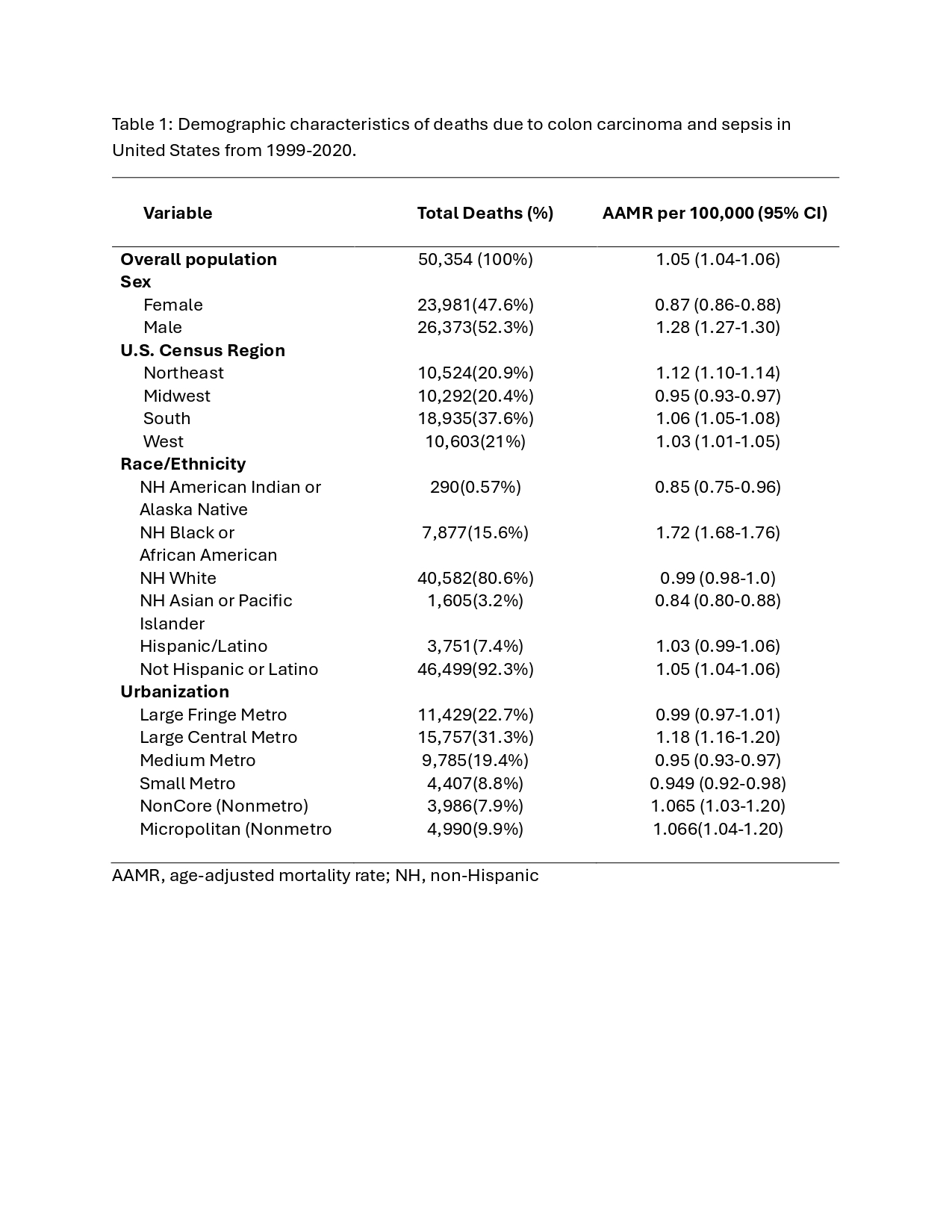
From 1999–2020, 50,354 deaths occurred (AAMR=1.05/100,000), with a decline from 1999–2012 (APC=-1.80, 95% CI: -2.18, -1.43). Black or African American individuals (AAMR=1.72) had the highest burden and largest decline (AAPC=-2.02, 95% CI: -2.39, -1.64), followed by White individuals (AAMR=0.99; AAPC=-1.11, 95% CI: -1.48, -0.74; 1999–2012: APC=-1.71, 95% CI: -2.11, -1.31; 2012–2020: stable). Asian or Pacific Islander (AAMR=0.84; AAPC=-1.10, 95% CI: -1.85, -0.35) and Hispanic or Latino individuals (AAMR=1.03; 2005–2020: APC=-0.98, 95% CI: -1.90, -0.06) also declined. Large fringe metro areas (AAMR=0.99; AAPC=-2.04, 95% CI: -2.45, -1.63) had the sharpest drop, followed by medium (AAMR=0.95; AAPC=-0.69, 95% CI: -1.06, -0.32) and small metro (AAMR=1.07; AAPC=-0.82, 95% CI: -1.27, -0.38), while rural noncore areas (AAMR=1.07; AAPC=0.21, 95% CI: -0.27, 0.69) rose slightly. Males showed a decline (AAMR=1.28; AAPC=-1.29, 95% CI: -1.52, -1.06); females (AAMR=0.87; AAPC=-1.17, 95% CI: -2.49, 0.17) did not. The Northeast (AAMR=1.12; AAPC=-2.90, 95% CI: -3.15, -2.64) led declines, followed by Midwest (AAMR=0.95; AAPC=-1.13, 95% CI: -1.49, -0.78) and West (AAMR=1.03; AAPC=-0.74, 95% CI: -1.14, -0.34). Maryland (AAPC=-3.88), New Jersey (-2.94), New York (-2.92), and Illinois (-1.61) improved; California, Texas, Florida, and Washington stayed stable.
Colon carcinoma-sepsis mortality fell from 1999–2020, but disparities remain in race/ethnicity (highest in Black or African American individuals), sex (stable in females), urbanization (rising rural trends), and region/state (stable in California, Texas). Interventions to improve rural and female healthcare access are needed.