
Monday Poster Session
Category: Colon


Grace C. Ramirez, MD
Baycare Health Systems, St. Joseph's Hospital
Tampa, FL
A 66-year-old woman with a history of hypertension, GERD, Barrett’s esophagus, and osteoporosis presented with decades-long gastrointestinal symptoms, including abdominal pain, bloating, nausea, vomiting, and diarrhea. Symptoms were intermittently triggered by foods such as alcohol and certain breads and seasonings but sometimes occurred spontaneously with nighttime awakenings. An elimination diet failed to identify consistent triggers and workups for common GI disorders, including celiac disease, were unremarkable.
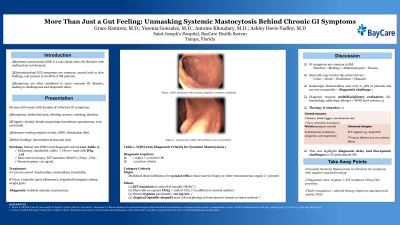
Endoscopic evaluation revealed duodenitis and colitis with histologic features raising suspicion for systemic mastocytosis with CD117+ for mast cells. A bone marrow biopsy later reinforced the diagnosis, demonstrating an activating KIT mutation. Tryptase levels were persistently elevated ( >20 ng/mL). These findings fulfilled both the major and minor diagnostic criteria for systemic mastocytosis, specifically the indolent variant.
After trials with multiple medications, the patient’s symptoms have been controlled with fexofenadine, montelukast, and famotidine. Other medications included Cromolyn, which was discontinued due to poor adherence, and a trial drug, Avapritinib, which was stopped due to lower extremity edema and weight gain.

