Monday Poster Session
Category: Colon

Sahil Sabharwal, MD
University of Arkansas for Medical Sciences
Fayetteville, AR
Goblet cell adenocarcinoma (GCA), previously termed goblet cell carcinoid, is a rare amphicrine tumor primarily of appendiceal origin, often found incidentally during for suspected appendicitis. It exhibits mucinous and neuroendocrine differentiation, and poorly defined due to its rarity and historical nomenclature variability. We will discuss GCA’s incidence as an incidental discovery secondary to two patient cases.
Here we will discuss two elderly males with incidentally found GCA.
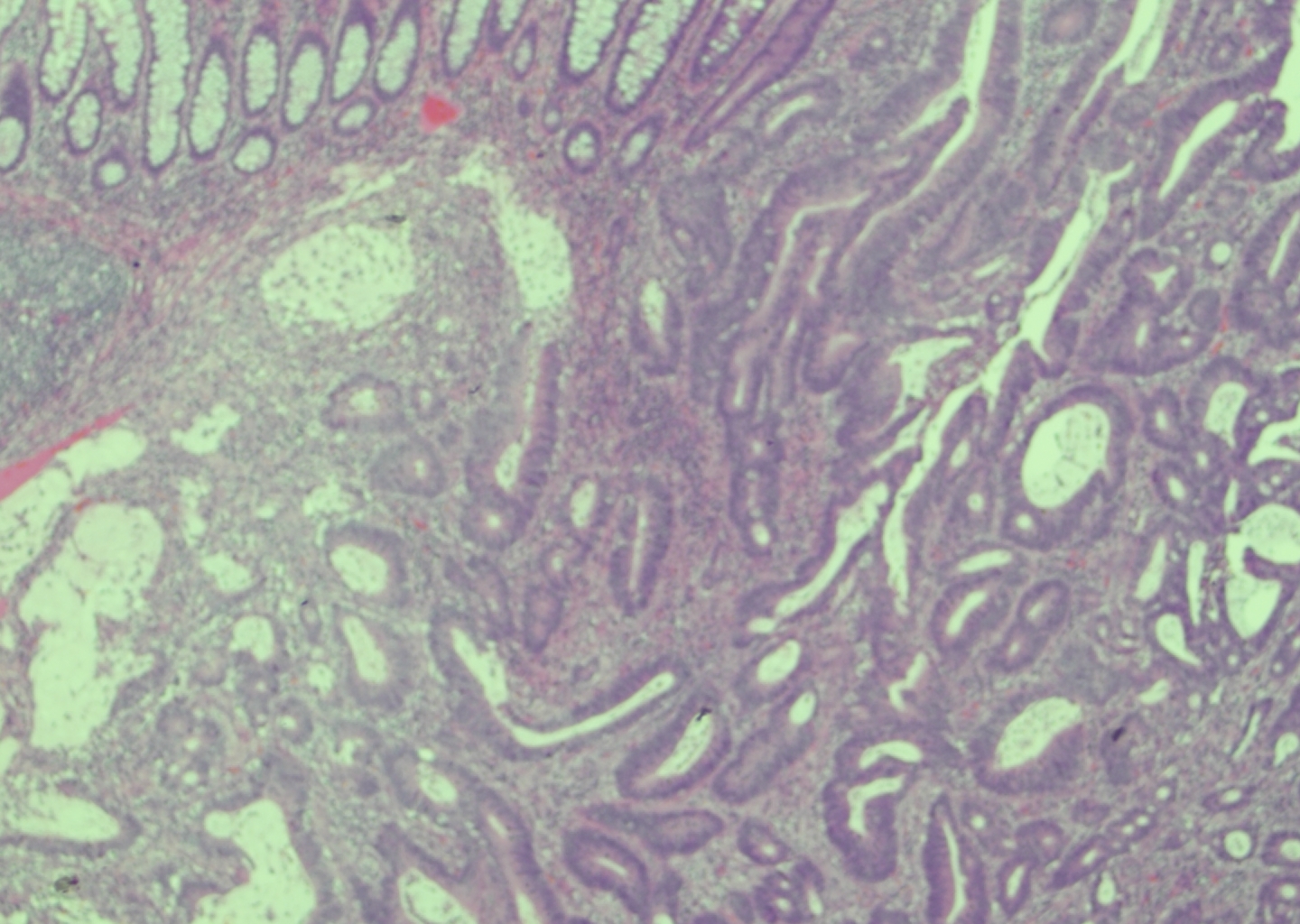
The first patient underwent laparoscopic right hemicolectomy with appendectomy and a laparotomy with resection of ischemic small bowel 6 weeks ago. Pathologic reports show colonic adenocarcinoma. However, during pathologic review, GCA was incidentally discovered found in association with the colonic adenocarcinoma (figure 1).
The second patient underwent appendectomy due to appendicitis. During pathologic review, the patient was incidentally found to have GCA (figure 2).
GCA has an overall incidence of 0.01–0.3 per 100,000 annually and constitutes less than 5% of appendiceal neoplasms. GCA typically occurs 0.3-0.9% of appendectomy specimens in patients with acute appendicitis or non-specific abdominal pain as an incidental finding. It has a subtle presentation often presenting as appendiceal wall thickening without distinct mass formation. Therefore, diagnosis is often made via postoperative histology. Preoperative imaging, such as CT scan, rarely identifies characteristic features, reinforcing incidental detection.
Case reports document GCA’s incidental discovery during appendectomies and, less commonly, colonoscopies revealing abnormal appendiceal orifices, which highlights the need for thorough histological examination, as standard grossing protocols may miss early GCA.
In 2019, the WHO classification standardized GCA as an adenocarcinoma with a 3-tier grading system. Incidental GCAs are often low-grade, with 5-year survival rates of 91–100% for stage I. High-grade or metastatic cases (10–50% at diagnosis) have poorer outcomes (14–22% for stage IV). Appendectomy suffices for low-grade GCA, but completion right hemicolectomy is recommended for higher-grade cases, with no current standardized guidelines for adjuvant therapy.
Due to GCA’s rarity, large-scale studies are scarce. Enhanced pathological protocols and awareness of GCA’s histological features are vital for detection. Prospective registries are needed to clarify incidental GCA’s incidence and optimize management.