P2244 - Identification of Pancreaticobiliary Maljunction and Resultant Gallbladder Cancer Using Endoscopic Retrograde Cholangiopancreatography (ERCP)-Endoscopic Ultrasound (EUS)
Introduction: A 76-year-old female patient with a medical history of hypertension, dementia, lupus, and fibromyalgia presented to the emergency department from her long-term care facility for elevated liver function tests (LFTs). At her facility, patient developed jaundice and scleral icterus, so her LFTs where checked with alanine aminotransferase (ALT) 177, aspartate aminotransferase (AST) 129, alkaline phosphatase (ALP) 620, and total bilirubin of 6. Daughter reports that patient also had unintentional weight loss and loss of appetite. This case will detail the subsequent workup and role of Endoscopic Retrograde Cholangiopancreatography (ERCP)-Endoscopic ultrasound (EUS) in diagnosing gallbladder cancer, which is typically found after surgical resection, in a patient found to have predisposing pancreaticobiliary maljunction (PBM).
Case Description/Methods: MRI Magnetic Resonance Cholangiopancreatography (MRCP), with and without contrast, was obtained which noted intrahepatic and extrahepatic biliary ductal dilation and abrupt truncation in the mid region of the common bile duct, along with a 3.1 cm mass within the gallbladder. Decision was then made to proceed with ERCP-EUS for biopsy.
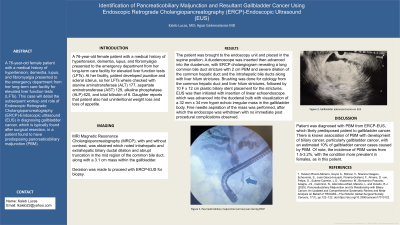
The patient was brought to the endoscopy unit and placed in the supine position. A duodenoscope was inserted then advanced into the duodenum, with ERCP cholangiogram revealing a long common bile duct stricture with 2 cm PBM and severe dilation of the common hepatic duct and the intrahepatic bile ducts along with liver hilum strictures. Brushing was done for cytology from the common hepatic duct and liver hilum strictures, followed by 10 F x 12 cm plastic biliary stent placement for the strictures. EUS was then initiated with insertion of linear echoendoscope which was advanced into the duodenal bulb with visualization of a 32 mm x 34 mm hyper echoic irregular mass in the gallbladder body. Fine needle aspiration of the mass was performed, after which the endoscope was withdrawn with no immediate post procedural complications observed.
Discussion: Patient was diagnosed with PBM from ERCP/EUS, which likely predisposed patient to gallbladder cancer and cholangiocarcinoma. There is known association of PBM with development of biliary cancer, particularly gallbladder cancer, with an estimated 10% of gallbladder cancer cases caused by PBM. Of note, the incidence of PBM varies from 1.5-3.2%, with the condition more prevalent in females, as in this patient.
Figure: Pancreaticobiliary maljunction seen with ERCP
Figure: Gallbladder adenocarcinoma on EUS
Disclosures:
Kaleb Lucas indicated no relevant financial relationships.
Agazi Gebreselassie indicated no relevant financial relationships.
Kaleb Lucas, MD1, Agazi Gebreselassie, MD2. P2244 - Identification of Pancreaticobiliary Malfunction and Resultant Gallbladder Cancer Using Endoscopic Retrograde Cholangiopancreatography (ERCP)-Endoscopic Ultrasound (EUS), ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.