Monday Poster Session
Category: Colon

Lefika Bathobakae, MD, MPH
St. Joseph's University Medical Center
Paterson, NJ
Horseshoe perianal abscess is a rare and severe form of anorectal sepsis that typically arises from cryptoglandular infection. Foreign body migration leading to deep perianal abscess formation is exceedingly rare, with a handful of cases reported to date.1,2 A fishbone-induced horseshoe abscess presents a diagnostic and therapeutic challenge due to its atypical etiology and deep anatomical spread. Herein, we present a rare case of a horseshoe perianal abscess caused by an ingested fishbone.
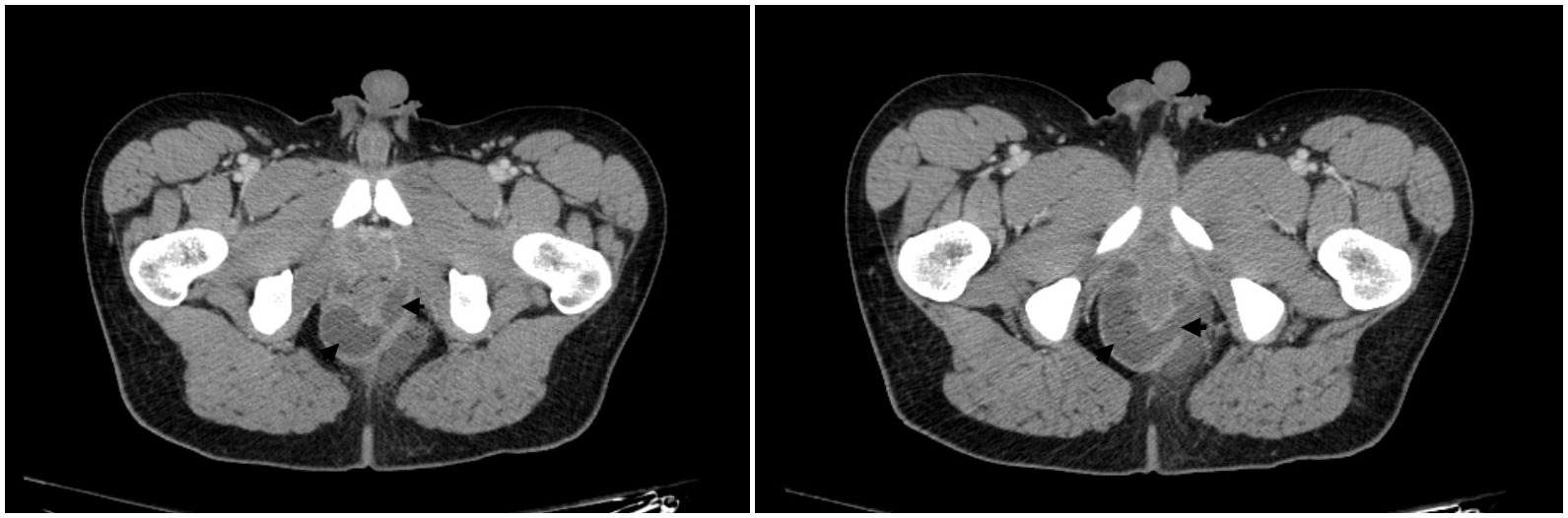
A 34-year-old man with a history of chronic constipation and prolapsing hemorrhoids presented to the ED for peri-rectal pain and fever. A month prior, the patient removed a large fishbone from his rectum and since then, he has been experiencing intermittent anorectal pain without hematochezia. He denied pelvic trauma, engaging in anoreceptive sex, a personal history of IBD or colorectal cancer. A digital rectal exam was notable for perirectal erythema, tenderness, and posterior fullness. Labs showed elevated CRP and ESR and leukocytosis. Contrast-enhanced CT of the pelvis revealed proctitis with large horse-shoe shaped perirectal/perianal abscess (Figure 1).
The patient was empirically treated with piperacillin-tazobactam for sepsis and underwent incision and drainage. On exam, the patient had cellulitic changes in the bilateral ischial rectal fossa, especially in the left side. Internal examination demonstrated an opening with spontaneous drainage of abscess at the left upper quadrant. Abscess was expressed as much as possible through the opening. Finger dissection was used to break up any loculations and all purulent material was expressed. A Penrose drain was placed and secured to the skin using 2-0 nylon. The patient had an uneventful post-operative course and was discharged on day six without further complications.
Fishbones, due to their sharp, rigid structure, can perforate the GI tract and migrate into adjacent soft tissues. In this case, the fishbone likely perforated the distal rectum and tracked into the deep postanal space, resulting in a complex horseshoe abscess. The absence of a clear ingestion history and the deep anatomical location made preoperative diagnosis particularly challenging. Management requires a high index of suspicion, careful surgical drainage, and complete removal of the foreign body to prevent recurrence.1–3 This case underscores the importance of considering atypical causes in recurrent or unusually severe anorectal sepsis.