Monday Poster Session
Category: Colon

Riddhi Machchhar, DO
Hackensack Meridian OUMC
Brick, NJ
IP remains an enigmatic condition in clinical practice, with no clear consensus on its etiology. While often incidental, the diagnosis requires careful differentiation from more common causes of free air in the abdomen, emphasizing the importance of thorough evaluation and management
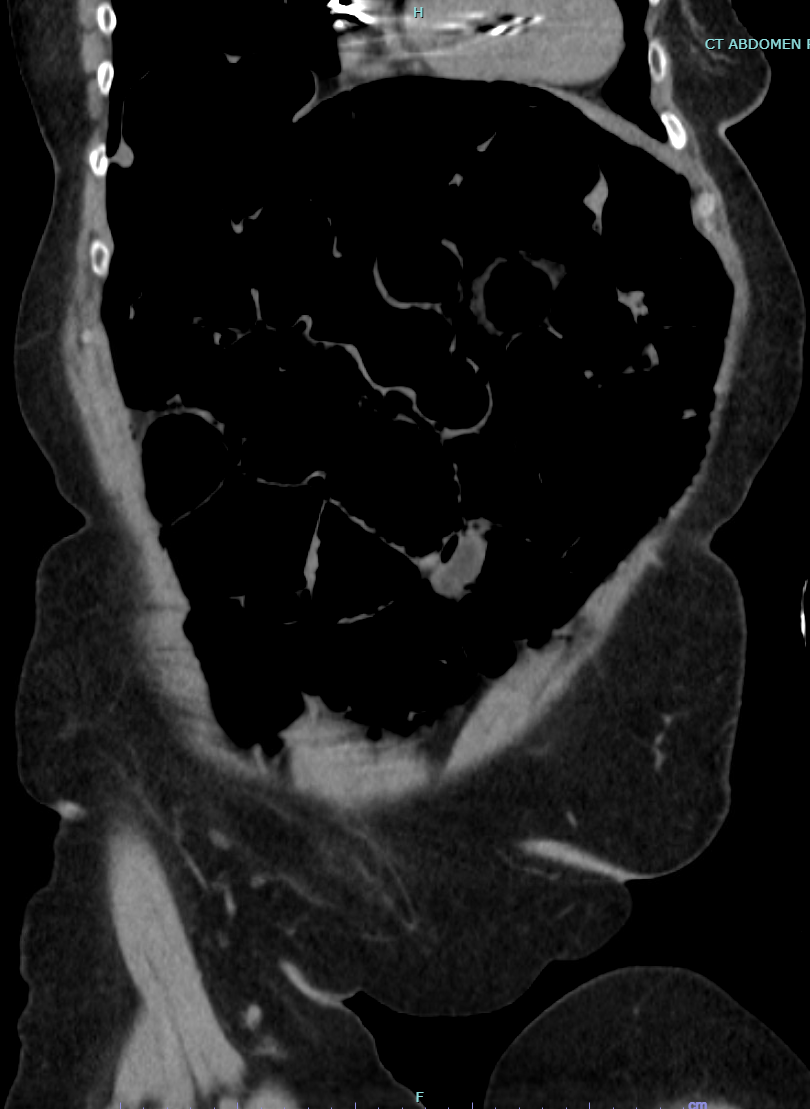
A 76 yo F w/ PMHx DM II, HLD, medullary thyroid cancer post-thyroidectomy, CHF presented to the ER after her Holter monitor revealed intermittent 3rd degree AVB. She was asymptomatic with no complaints. On presentation, she was stable, with normal vitals except for occasional dips in HR to the 40s. A CXR revealed pneumomediastinum, prompting further imaging. A CT scan showed not only pneumomediastinum but also pneumoperitoneum in the upper abdomen, raising concern for a possible perforated viscus.
She was admitted to the ICU for monitoring with placement of a temporary TVP pending PPM placement. Despite the concerning imaging, her clinical exam showed a soft, non-tender abdomen with no signs of acute distress, and her lab work remained stable.
Gen surg performed a diagnostic ex-lap, which revealed no perforation, though the presence of sevoflurane in the abdomen suggested an abnormal communication between the thorax and abdomen, potentially from a ruptured mediastinal bleb. The ex-lap ruled out a perforated viscus or colon.
A PPM was successfully placed, and the patient was discharged in stable condition on oral AC, with plans for close follow-up and monitoring.