Monday Poster Session
Category: Colon

Keshavi Mahesh, MD
Broward Health North
Pompano Beach, FL
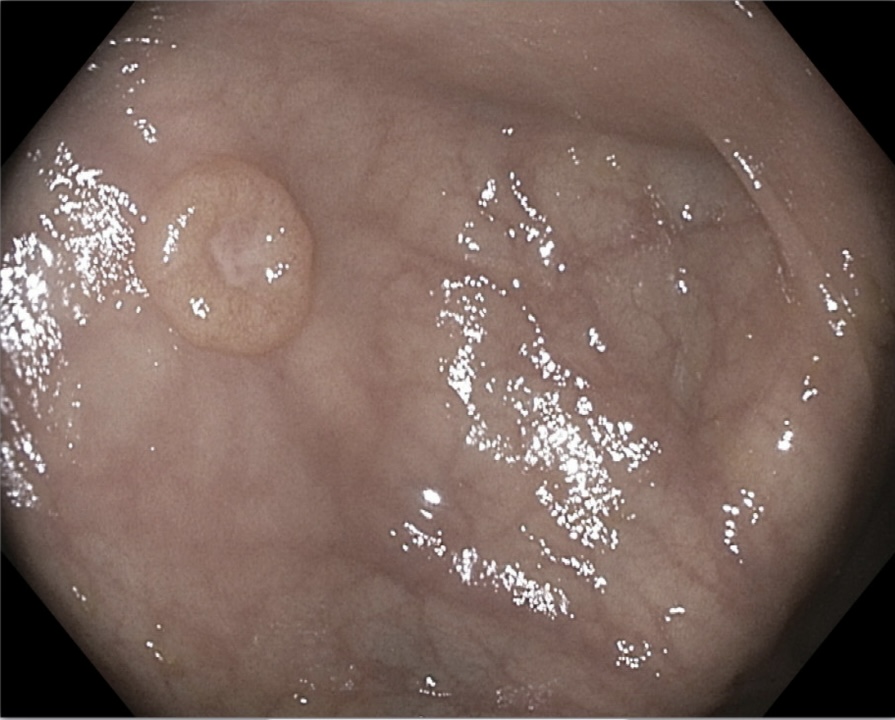
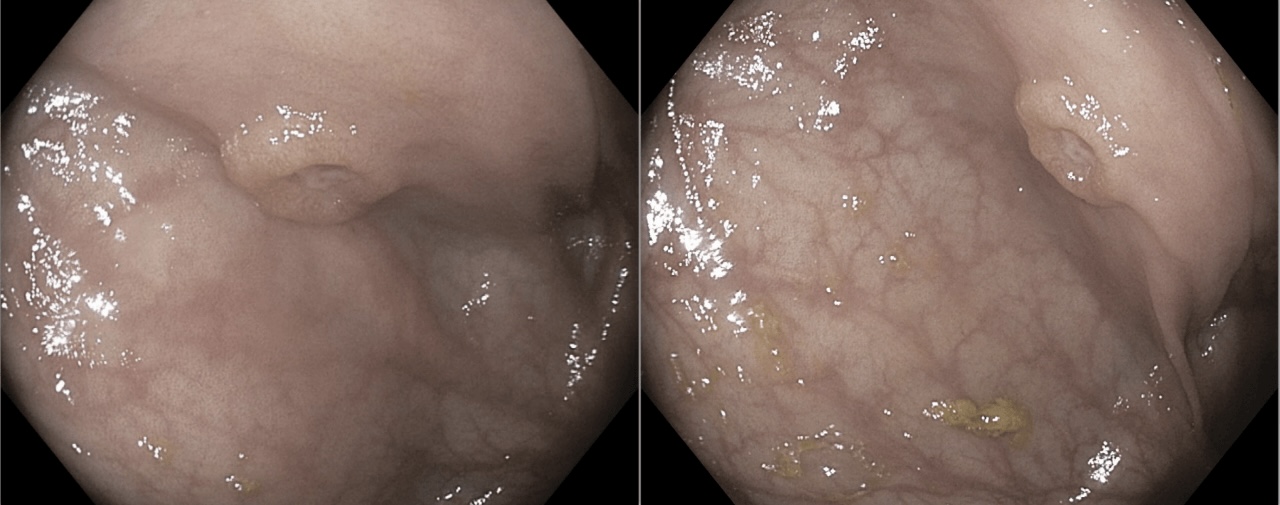
A 66-year-old female with a history of pulmonary NET status post left thoracotomy and pneumonectomy presented to our clinic for routine colon cancer screening. She had remained under surveillance until disease recurrence in the lung was detected on NETSPOT PET and confirmed via biopsy. The patient was initiated on octreotide LAR and monitored with serial serotonin and chromogranin A levels. She denied abdominal pain, melena, or hematochezia, and had no family history of colorectal cancer. Colonoscopy revealed a 1 cm circumferential, umbilicated lesion with a central depression located in the cecum. The lesion was removed using cold biopsy forceps and submitted for histopathological evaluation. Final pathology demonstrated a well-differentiated NET, WHO grade 2, with immunohistochemical staining positive for CKAE1/3, synaptophysin, and chromogranin, and Ki-67 index of approximately 10%. The patient was informed of the results and referred to oncology for further management.
Metastatic spread of pulmonary neuroendocrine tumors to the gastrointestinal tract is rare, with involvement of the colon, and particularly the cecum, being an exceptionally uncommon occurrence. Given the indolent nature of many NETs, metastasis may remain clinically silent and detected only through imaging or endoscopic evaluation. These lesions can closely mimic primary colorectal lesions, posing diagnostic challenges. Due to the limited number of reported cases in the literature, this case contributes valuable insight into an unusual pattern of metastatic disease. It highlights the importance of maintaining clinical vigilance during routine screening of NET patients, as early identification of atypical metastatic sites facilitates timely diagnosis and comprehensive patient management.