
Monday Poster Session
Category: Colon
Taofeek Kolade, MD, MBA, MPH
Bayonne Medical Center
Bayonne, NJ
Burkitt lymphoma is a highly aggressive B-cell non-Hodgkin lymphoma characterized by the translocation and dysregulation of the MYC gene on chromosome 8, leading to rapid tumor growth. It presents in three clinical forms: endemic, typically seen in African children with jaw tumors; sporadic, often manifesting as abdominal masses in Western populations; and immunodeficiency-associated, primarily affecting HIV-positive individuals. While sporadic Burkitt lymphoma is more common in younger patients, it can also present in older adults with gastrointestinal (GI) symptoms. Due to its rapid progression, early diagnosis and treatment are essential.
A 77-year-old female with a history of hypertension and hypothyroidism presented with one week of diffuse abdominal pain, constipation, oliguria, and bloody bowel movements. She was hemodynamically stable but exhibited diffuse abdominal tenderness. Laboratory results revealed hemoglobin of 10.1 g/dL, lactate of 6.9 mmol/L, BNP of 1720 pg/mL, creatinine of 1.3 mg/dL, and BUN of 21 mg/dL.
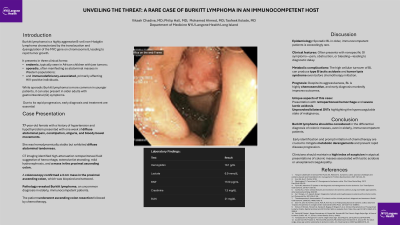
CT imaging identified high-attenuation retroperitoneal fluid suggestive of hemorrhage, extensive fat stranding, mild hydronephrosis, and a mass in the proximal ascending colon. A colonoscopy confirmed a 3 cm mass in the proximal ascending colon, which was biopsied and tattooed. Pathology revealed Burkitt lymphoma, an uncommon diagnosis in elderly, immunocompetent patients. The patient underwent ascending colon resection followed by chemotherapy.
Although sporadic Burkitt lymphoma is rare in older adults, it should be considered in immunocompetent elderly patients with abdominal masses and GI symptoms. The disease typically responds well to chemotherapy, but its high metabolic activity can lead to complications such as tumor lysis syndrome and type B lactic acidosis. In this case, persistent metabolic acidosis was attributed to the lymphoma’s high cellular turnover. Additionally, the patient developed unprovoked deep vein thromboses (DVTs) in the right peroneal and left soleal veins, likely secondary to a malignancy-induced hypercoagulable state, necessitating IVC filter placement.
This case emphasizes the importance of including Burkitt lymphoma in the differential diagnosis of colonic masses, even in older populations. Early identification is critical, as delayed diagnosis can lead to severe metabolic complications and rapid disease progression. A comprehensive workup and timely intervention remain essential to optimizing outcomes.
