Monday Poster Session
Category: Colon

Abdelrhman Refaey, MD
Division of Gastroenterology and Liver Disease, Department of Medicine, George Washington University School of Medicine and Health Sciences
Teaneck, NJ
Cystic lymphangiomas are rare benign vascular malformations that can occur anywhere in the body. The most common sites are the neck and axilla (95%), with 5% occurring in the abdomen and mediastinum. Colorectal lymphangiomas typically present as incidental findings during colonoscopy, accounting for < 1% of colonic cystic lesions. Endoscopic ultrasound (EUS) can accurately diagnose these lesions without requiring more invasive procedures. Given the benign nature of these lesions, intervention is typically not required. We present an unusual case of a sigmoid colon subepithelial cystic lesion identified during a screening colonoscopy that was subsequently identified as a cystic lymphangioma.
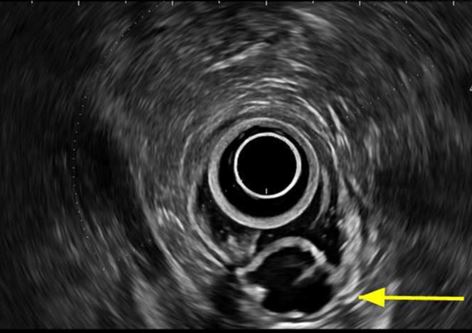
A 45-year-old man with gastroesophageal reflux and asthma underwent a screening colonoscopy. He had no gastrointestinal symptoms. Physical exam was unremarkable. A colonoscopy revealed a 2 cm non-obstructing cystic lesion in the sigmoid colon. A subsequent lower EUS identified a well-defined, thin-walled, oval, anechoic lesion with septae measuring 2 cm in the sigmoid colon. The lesion originated from the submucosa with an intact muscularis propria without Doppler flow, consistent with a cystic lymphangioma. Given the benign nature of the lesion, a biopsy was not performed. No further intervention was required.
Gastrointestinal cystic lymphangiomas are uncommon and rarely involve the colon. They are typically asymptomatic and discovered incidentally. EUS has a critical role in diagnosing these lesions and is a sufficient diagnostic tool. They appear as well-defined, thin-walled, anechoic cystic lesions with septations, intact muscularis propria, and no Doppler flow. Biopsies are unnecessary, since there is the potential for infectious complications. It is critical to distinguish cystic lymphangiomas from clinically significant mimickers that can include gastrointestinal stromal tumors, cystic teratomas, or metastatic cysts of ovarian or pancreatic origin. While other lesions may require surgical intervention, cystic lymphangiomas are managed conservatively unless symptomatic. Rare cases of abdominal pain, bleeding, alteration in bowel habits, and intussusception have been described, but the infrequency of symptoms does not warrant prophylactic surgical or endoscopic resection of asymptomatic lesions. This rare case of a colonic cystic lymphangioma reinforces the importance of recognizing the benign nature of this lesion to avoid unnecessary interventions.