Saint Michael's Medical Center, New York Medical College Newark, NJ
Mohamed Eldesouki, MD1, Ahmed Ibrahim, MD2, Mohammed Y. Youssef, MD3, Ahmed Salem, MD4, Hazem Abosheaishaa, MD5, Omar Alkasabrah, MD6, Anas A. Elsaka, MD7, Mona A. Ali, MD7, Sherif E. Elhanafi, MD8 1Saint Michael's Medical Center, New York Medical College, Newark, NJ; 2Medical University of South Carolina, Charleston, SC; 3Hunt Regional Medical Center, Greenville, TX; 4Maimonides Medical Center, Brooklyn, NY; 5Mount Sinai West, Icahn School of Medicine at Mount Sinai, Queens, NY; 6Landmark Medical Center, Woonsocket, RI; 7Mansoura University, Mansoura, Ad Daqahliyah, Egypt; 8Texas Tech University Health Sciences Center, El Paso, TX
Introduction: Bariatric surgeries are widely utilized for obesity management, however, their impact on the risk of developing Barrett’s esophagus (BE) remains uncertain. The aim of this study was to evaluate the long-term risk of BE after bariatric surgery using a large real-world cohort.
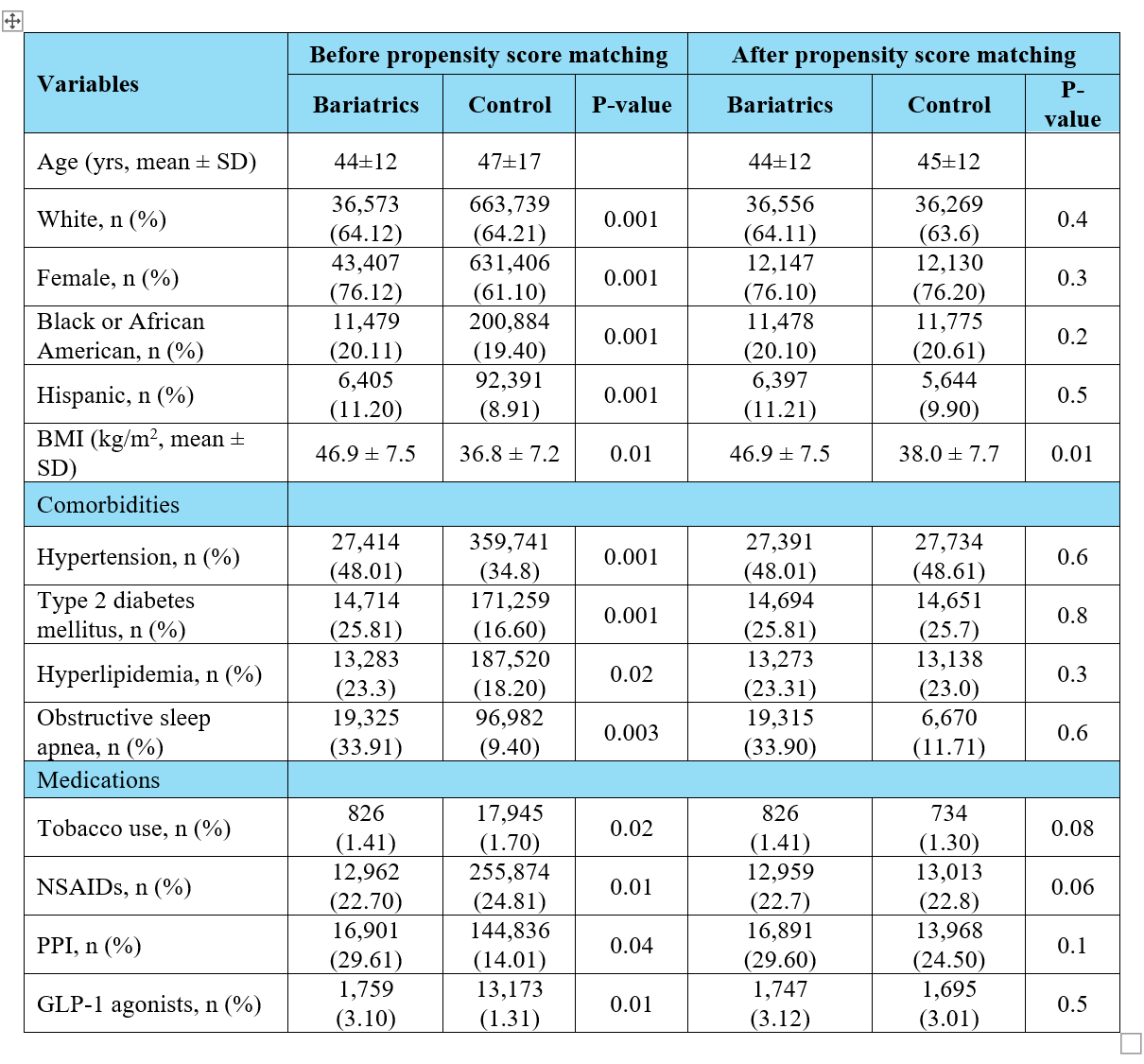
Results: A total of 58,910 patients underwent bariatric surgeries (31,228 sleeve, 27,682 gastric bypass), while 1,049,231 patients were in the control group before PSM. After matching, a total of 57,035 patients remained in each group (Table 1).
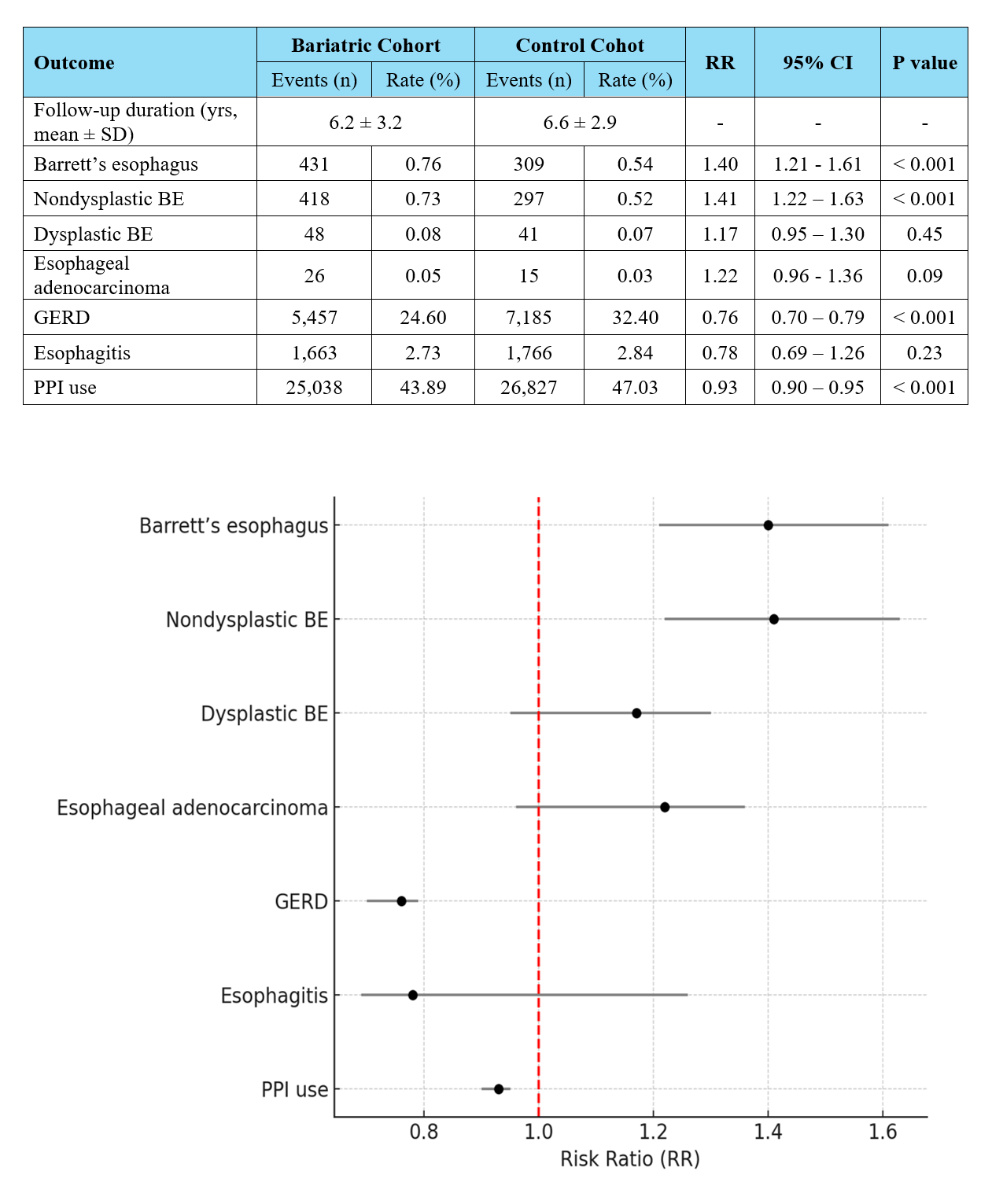
Bariatric surgery was associated with a higher incidence of Barrett’s esophagus compared to the control group (0.8% vs 0.5%; RR 1.39, 95 % CI 1.207 – 1.618, p< 0.001). Nondysplastic BE was significantly higher in the bariatric surgeries group (0.8 % vs 0.4 %; RR 1.77, 95 % CI 1.38 – 2.27, p< 0.001), however, no significant increases were noted in dysplastic BE (0.07 % vs 0.05 %; RR 1.60, 95 % CI 0.73–3.53), esophageal adenocarcinoma (0.05% vs 0.026%; RR 1.73, 99% CI 0.92 –3.37), and esophagitis (RR 0.78, 95 % CI 0.69– 1.12, p< 0.5).
Compared to obese controls, bariatric surgery patients had lower risk of reflux-mediated outcomes: GERD (24.04% vs 26.61%; RR 0.91, 95 % CI 0.84–0.93, p< 0.001), and need for PPI use (35.2 % vs 42.0 %; RR 0.84, 95 % CI 0.81–0.87, p< 0.001) (Table 2, Figure 1).
Discussion: In this large real-world cohort study, the risk of Barrett’s esophagus was higher in patients who underwent bariatric surgeries; however, bariatric surgeries were associated with substantial reductions in the development of GERD and PPI utilization. Prospective studies and tailored surveillance strategies for post-bariatric patients are warranted.
Figure: Table 1. Patients' demographics and clinical features before and after propensity score matching. Abbreviations- BMI: body mass index; NSAIDs: non-steroidal anti-inflammatory drugs; PPI: proton pump inhibitors; GLP-1: glucagon-like peptide-1.
Figure: Table 2. Clinical outcomes of the baratric surgery cohort vs. control. Figure. Forest plot depicting the clinical outcomes of the bariatric surgery group compared to the control. Abbreviations- BE: Barrett's esophagus; GERD: gastroesophageal reflux disease; PPI: proton pump inhibitors
Disclosures:
Mohamed Eldesouki indicated no relevant financial relationships.
Ahmed Ibrahim indicated no relevant financial relationships.
Mohammed Y. Youssef indicated no relevant financial relationships.
Ahmed Salem indicated no relevant financial relationships.
Hazem Abosheaishaa indicated no relevant financial relationships.
Omar Alkasabrah indicated no relevant financial relationships.
Anas Elsaka indicated no relevant financial relationships.
Mona Ali indicated no relevant financial relationships.
Sherif Elhanafi indicated no relevant financial relationships.
Mohamed Eldesouki, MD1, Ahmed Ibrahim, MD2, Mohammed Y. Youssef, MD3, Ahmed Salem, MD4, Hazem Abosheaishaa, MD5, Omar Alkasabrah, MD6, Anas A. Elsaka, MD7, Mona A. Ali, MD7, Sherif E. Elhanafi, MD8. P0621 - Increased Risk of Barrett’s Esophagus After Bariatric Surgery: A Propensity-Matched Analysis of 57,035 Patients, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.