Sunday Poster Session
Category: Colon
Ahmed Al Mubaid, DO
Franciscan Health Olympia Fields
Olympia Fields, IL
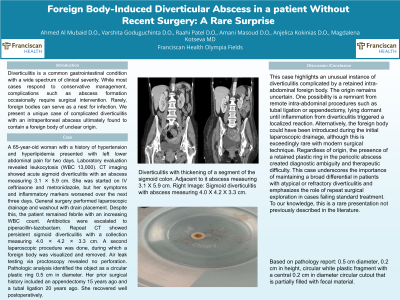
A 65-year-old woman with a history of hypertension and hyperlipidemia presented with left lower abdominal pain for two days. Laboratory evaluation revealed leukocytosis (WBC 13,000). CT imaging showed acute sigmoid diverticulitis with an abscess measuring 3.1 × 5.9 cm. She was started on IV ceftriaxone and metronidazole, but her symptoms and inflammatory markers worsened over the next three days. General surgery performed laparoscopic drainage and washout with drain placement. Despite this, the patient remained febrile with an increasing WBC count. Antibiotics were escalated to piperacillin-tazobactam. Repeat CT showed persistent sigmoid diverticulitis with a collection measuring 4.0 × 4.2 × 3.3 cm. A second laparoscopic procedure was done, during which a foreign body was visualized and removed. Air leak testing via proctoscopy revealed no perforation. Pathologic analysis identified the object as a circular plastic ring 0.5 cm in diameter. Her prior surgical history included an appendectomy 15 years ago and a tubal ligation 20 years ago. She recovered well postoperatively.
This case highlights an unusual instance of diverticulitis complicated by a retained intra-abdominal foreign body. The origin remains uncertain. One possibility is a remnant from remote intra-abdominal procedures such as tubal ligation or appendectomy, lying dormant until inflammation from diverticulitis triggered a localized reaction. Alternatively, the foreign body could have been introduced during the initial laparoscopic drainage, although this is exceedingly rare with modern surgical technique. Regardless of origin, the presence of a retained plastic ring in the pericolic abscess created diagnostic ambiguity and therapeutic difficulty. This case underscores the importance of maintaining a broad differential in patients with atypical or refractory diverticulitis and emphasizes the role of repeat surgical exploration in cases failing standard treatment. To our knowledge, this is a rare presentation not previously described in the literature.