
Sunday Poster Session
Category: Colon

Sindhuja Giridharan, MD
Nassau University Medical Center
East Meadow, New York
Endoscopic biliary stents are placed to relieve obstruction secondary to CBD stones, strictures and malignant obstruction. Common complications include stent occlusion and migrations. Perforation due to dislodged stent is a rare complication. The most common site of a migrated biliary stent is the duodenum, whereas complications in the rest of the small intestine or colon are rare. Routine prosthesis removal is done in 3 months but can be extended to 6 months.
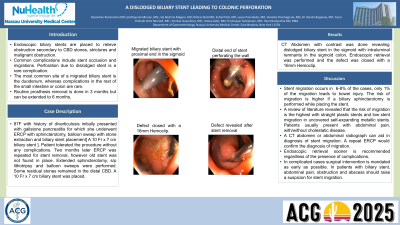
87F with history of diverticulosis initially presented with gallstone pancreatitis for which she underwent ERCP with sphincterotomy, balloon sweep with stone extraction and biliary stent placement[ A 10 Fr x 7 cm biliary stent ]. Patient tolerated the procedure without any complications. Two months later ERCP was repeated for stent removal, however old stent was not found in place. Extended sphincterotomy, s/p lithotripsy and balloon sweeps were performed. Some residual stones remained in the distal CBD. A 10 Fr x 7 cm biliary stent was placed. CT Abdomen with contrast was done revealing dislodged biliary stent in the sigmoid with intraluminal remnants in the sigmoid colon. Endoscopic retrieval was performed and the defect was closed with a 16mm Hemoclip.
Stent migration occurs in 6-8% of the cases, only 1% of the migration leads to bowel injury. The risk of migration is higher if a biliary sphincterotomy is performed while placing the stent. A review of literature revealed that the risk of migration is the highest with straight plastic stents and low stent migration in uncovered self-expanding metallic stents. Patients usually present with abdominal pain, with/without cholestatic disease. A CT abdomen or abdominal radiograph can aid in diagnosis of stent migration. A repeat ERCP would confirm the diagnosis of migration. Endoscopic retrieval sooner is recommended regardless of the presence of complications. In complicated cases surgical intervention is mandated as early as possible. In patients with biliary stent, abdominal pain, obstruction and abscess should raise a suspicion for stent migration.